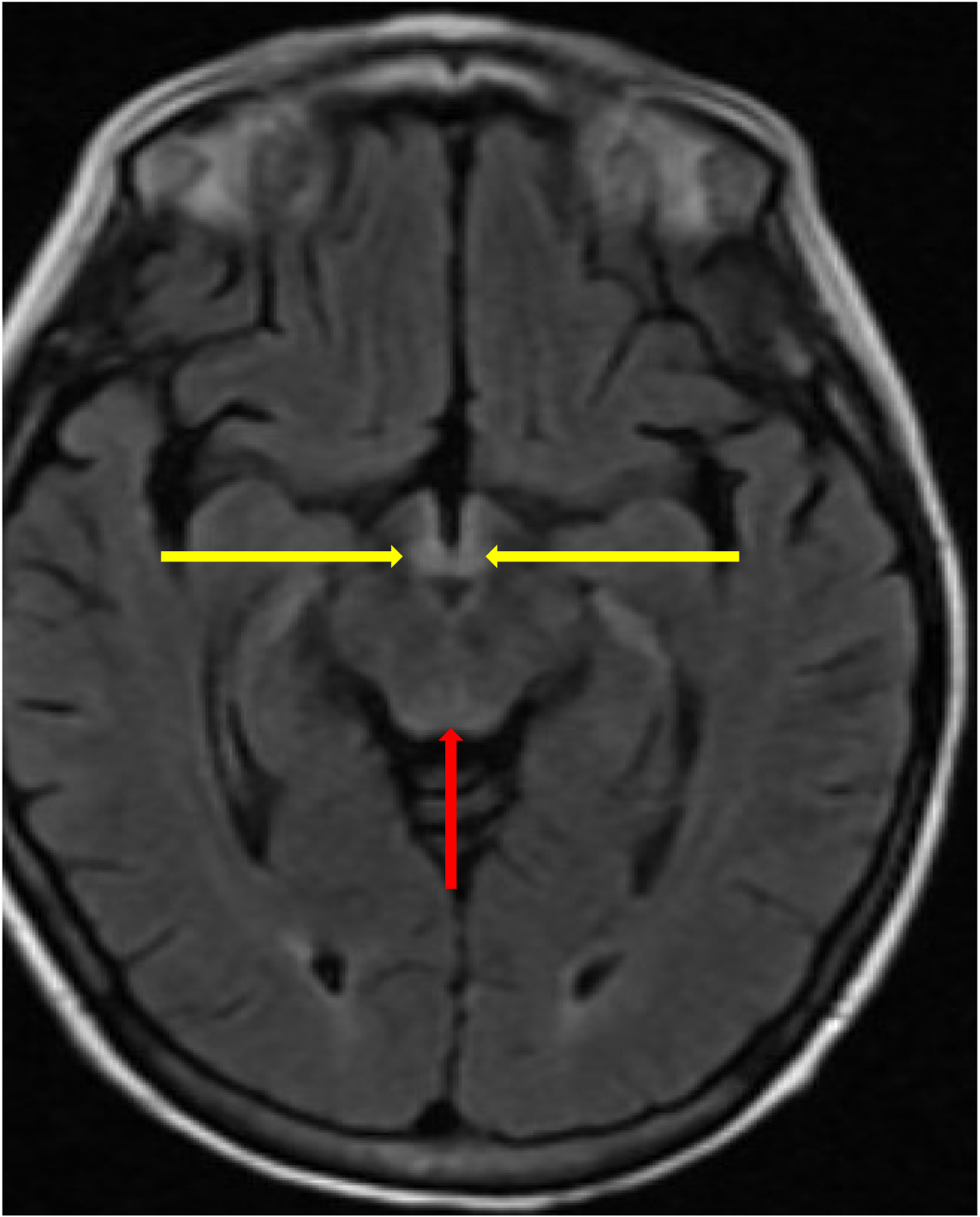
Case Presentation: A 40-year-old female presented to the emergency department with 4 days of unsteady gait, somnolence, and confusion. Her history included atrial fibrillation, depression, and Degos disease complicated by chronic malabsorption, pain, and jejunal perforations s/p ileocecectomy with total parenteral nutrition (TPN) dependence. She did not drink alcohol. Additional history revealed she switched to oral thiamine replacement from intravenous (IV) formulation 3 months prior.She was afebrile with normal vitals. She was encephalopathic with nystagmus and ataxia. Labs showed hypokalemia, hypoalbuminemia, and deficiencies of vitamins B6 and D, zinc, and selenium. She had a normal CBC, CMP, methylmalonic acid, thiamine (after supplementation), copper, manganese, carnitine, free T4, ammonia, and vitamins A, E, and K. HIV serologies were negative. She was admitted and started high dose IV thiamine. Infectious, autoimmune, and paraneoplastic work-up was negative. Brain MRI showed symmetric T2 FLAIR hyperintensity of the mamillary bodies, tegmentum, and cerebral aqueduct, characteristic of Wernicke’s encephalopathy (Figure 1).With high dose IV thiamine, her nystagmus and ataxia resolved, but some disorientation and visual hallucinations persisted at time of discharge. Although initially concerning for Degos disease with neurologic involvement, the history, exam, labs, imaging findings, and improvement with high dose thiamine supported Wernicke’s encephalopathy.
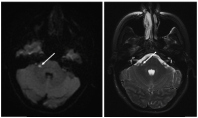
Discussion: Degos disease, or systemic malignant atrophic papulosis, is a microvascular thrombotic condition primarily of the brain, skin, and gastrointestinal tract.[1] With less than 200 confirmed cases worldwide, the etiology is unknown.[2] Major organ involvement has a poor prognosis and is often fatal within 2 years of diagnosis.[3] In 47% of patients, Degos disease presents with gastrointestinal complications such as dyspepsia, abdominal pain, bleeding, or bowel perforation. [3] CNS involvement, such as cranial nerve deficits or polyradiculoneuropathy, is seen in 20-60% of cases.[4] Kidney, lung, eye, heart, and pancreatic involvement can also occur.[5] Diagnosis is clinical with pathognomonic histopathologic skin biopsy findings of connective tissue necrosis and microvascular occlusion.[2] Treatment options are limited; however fibrinolytic and immunologic therapies can improve symptoms in some patients but worsen the condition in others.[2] Anticoagulants have also shown skin lesion regression in some cases.[2]At presentation, concern was highest for Degos disease with CNS involvement. However, her brain MRI lacked findings reported in Degos disease, including diffusion along margins of the brainstem, cortical or subcortical foci, spinal lesions, or leptomeningeal enhancement (Figure 2).[4] The clinical presentation and brain MRI were characteristic of Wernicke’s encephalopathy from inadequate thiamine supplementation (a consequence of Degos associated malabsorption). Her improvement with thiamine supplementation confirmed the diagnosis.
Conclusions: Wernicke’s encephalopathy in a patient with Degos disease is not documented in the literature. This case presented a diagnostic challenge and offered a valuable learning experience about a rare neurological condition within the context of an even rarer systemic disease.