Case Presentation:
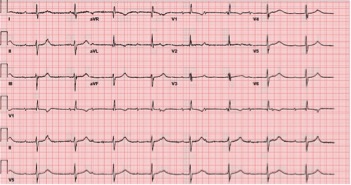
A 47 year-old female with hypertension, dyslipidemia, and diabetes presented with two weeks of dyspnea. An ECG a year prior showed normal sinus rhythm. The rhythm strip from a transthoracic echocardiogram incidentally showed complete heart block. An ECG confirmed new persistent third degree AV block. A left heart catheterization ruled out coronary artery disease and workup for other reversible causes such as lyme disease, syphilis, autoimmune (ANA, ANCA, CCP), and thyroid disease was negative. A transesophageal echocardiogram was negative for valvular abnormalities. A cardiac MR was nondiagnostic for an infiltrative process, but showed late gadolinium enhancement in the inferolateral septum, indicative of nonspecific scarring. A nuclear myocardial perfusion study then showed abnormal perfusion along the anterior wall and areas of late enhancement, again nonspecific findings for cardiac sarocoidosis (CS). Thus, a cardiac positron emission tomography scan was performed showing multiple hypermetabolic regions within the heart consistent with a sarcoid pattern as well as mediastinal lymphadenopathy. In collaboration with Rheumatology, a diagnosis of “highly probable” primary cardiac sarcoidosis was made without histology and she was started on methotrexate. Electrophysiology implanted a dual chamber pacemaker with moderate symptomatic improvement with ICD placement subsequently planned.
Discussion:
Cardiac involvement must always be assessed in sarcoidosis, but in rare cases may precede other organ involvement. Disagreement exists on how best to diagnose and categorize CS. Histologic diagnosis may be difficult – particularly in isolated CS where biopsy carries higher risk. Further controversy exists over how clinicians can best utilize and navigate new modalities like CMR and cardiac PET. Meanwhile, diagnostic inertia can delay initiation of immunosuppressive therapy as well as implantation of appropriate cardiac devices. In this case, common causes of her heart block were ruled out via lab testing and imaging. A probable diagnosis was ruled in by major (AV block) and minor criteria (perfusion defects, late enhancement on MR, abnormal echocardiography) using the 2006 modified Japanese criteria. As in this case, the diagnostic difficulty of CS will yield only a frustratingly probable diagnosis but early treatment is essential to reduce morbidity and mortality.
Cardiac sarcoidosis (CS) may be present in 5 to 25 percent of sarcoidosis and causes significant morbidity and mortality. Its effects are often clinically silent and may precede other organ involvement. Further, CS manifests as diverse pathologies such as arrhythmias, heart failure, sudden cardiac death, valvular dysfunction, and pericardial disease. While sarcoid is frequently on the differential as a great imitator, definitive diagnosis remains problematic despite advanced cardiac imaging modalities like magnetic resonance and dedicated cardiac PET. Given phenotypic variability, lack of a gold standard, nonspecific imaging findings, and divergence among guidelines and position statements, diagnosis of primary CS, can be especially difficult and requires a high index of suspicion.
Conclusions:
Internists must consider cardiac sarcoidosis in the differential for any new unexplained cardiac abnormalities, particularly ECG findings in younger adults, and in cases of high probability, navigate a careful and thorough diagnostic approach.