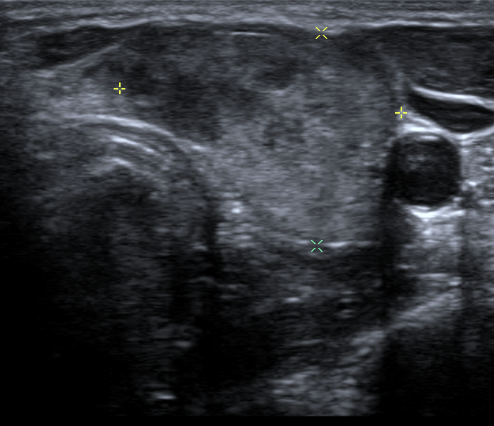
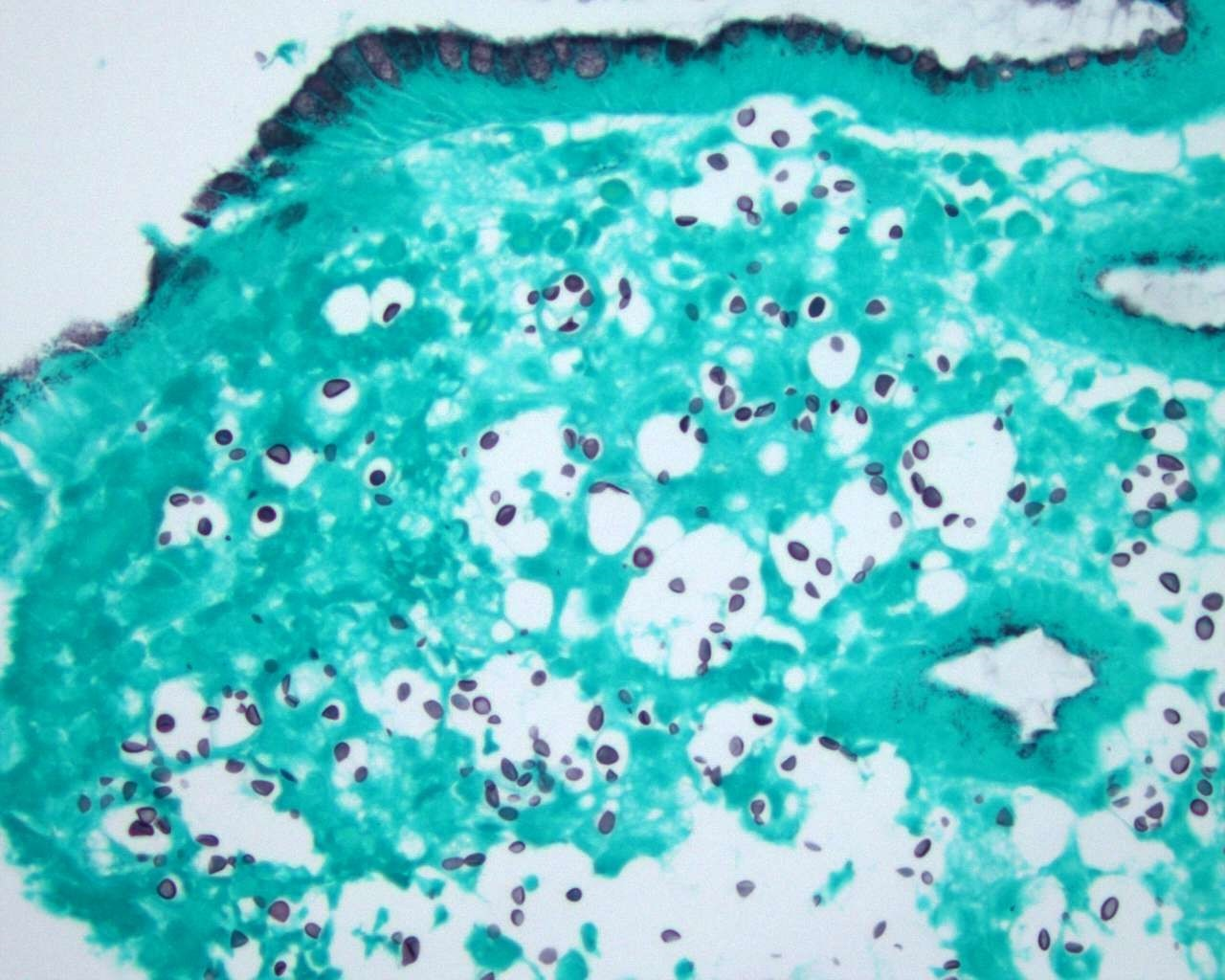
Case Presentation: A 30 year-old female with AIDS presented with three weeks of headache, dry cough, odynophagia, vomiting, fatigue and weight loss. She had a history of cryptococcal meningitis requiring lumbo-peritoneal drain four years prior but was lost to follow up, with non-adherence to maintenance and antiretroviral therapy. She had normal vital signs and appeared cachectic with oropharyngeal candidiasis and a tender, palpable left thyroid nodule. Laboratory evaluation revealed CD4 count < 20 and HIV viral load of 33,600 copies/mL, serum cryptococcus antigen titer of 1:65,500 and TSH of 4.0. Lumbar puncture revealed positive cerebrospinal fluid (CSF) titer of cryptococcus of 1:32,768 and was eventually cultured for cryptococcus neoformans. CT of the chest showed miliary pattern micronodularity throughout the lungs. Patient underwent bronchoscopy with bronchoalveolar lavage culture positive for cryptococcus neoformans. To evaluate the odynophagia, a CT of the soft tissue neck and xray esophagram revealed a para-esophageal 0.9 cm rim-enhancing fluid collection with adjacent walled-off lumen at the level of C7-C8, a mildly enlarged thyroid gland, and a 3 cm left thyroid nodule. An endoscopy ruled out a gross esophageal perforation but incidentally revealed a 12mm cratered ulcer in the gastric body with biopsies from the fundus, which showed cryptococcus. A thyroid ultrasound revealed a dominant heterogeneous nodule measuring 3.8 x 2.4 x 1.6 cm with hyperemia and calcifications. Fine needle aspiration biopsy revealed thyroid cryptococcus. We initiated induction therapy with Amphotericin B and Flucytosine. Amoxicillin-clavulonic acid treated the para-esophageal abscess and CT of the neck confirmed the resolution of abscess.
Discussion: Cryptococcus neoformans is an AIDS-defining illness in patients with a CD4 count < 200. It can result in disseminated disease to any organ system, with the most common sequela being the CNS and lungs. Gastrointestinal tract and more notably, thyroid involvement is rarely described. Gastric cryptococcus has generally been found in postmortem autopsies, but has been reported to clinically present as abdominal distension with back pain (1), melena (2), and odynophagia (3,4) with diagnosis made by endoscopy. There are very few previously reported cases of thyroid cryptococcal infection with majority also being postmortem autopsy findings (5–8). Other variable presentations include a triphasic clinical course similar to that of subacute thyroiditis (9,10), goiter (11), abscess (12) and thyroid enlargement (13,14). We report a case with an unusual presentation of disseminated cryptococcal infection in an AIDS patient with odynophagia and vomiting found to have a para-esophageal abscess, infectious thyroiditis with normal thyroid function tests, and gastric cryptococcus. In this case, endoscopy confirmed the presence of cryptococcus in the gastric fundus and fine-needle aspiration biopsy uncovered cryptococcal organisms in the thyroid. The diagnosis of disseminated cryptococcus with gastric and thyroid involvement led to induction therapy with Amphotericin B and Flucytosine.
Conclusions: We conclude that gastric and thyroid involvement is an under-recognized phenomenon of disseminated cryptococcus and may be overlooked if infectious etiologies are not considered. Suspicion must be high in an immunocompromised patient with odynophagia and a thyroid nodule and warrants further investigation by endoscopy and fine needle aspiration biopsy.