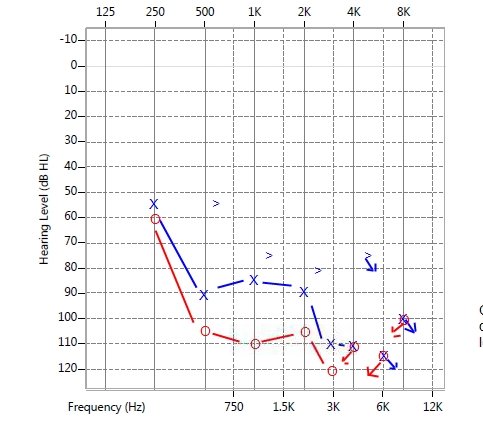
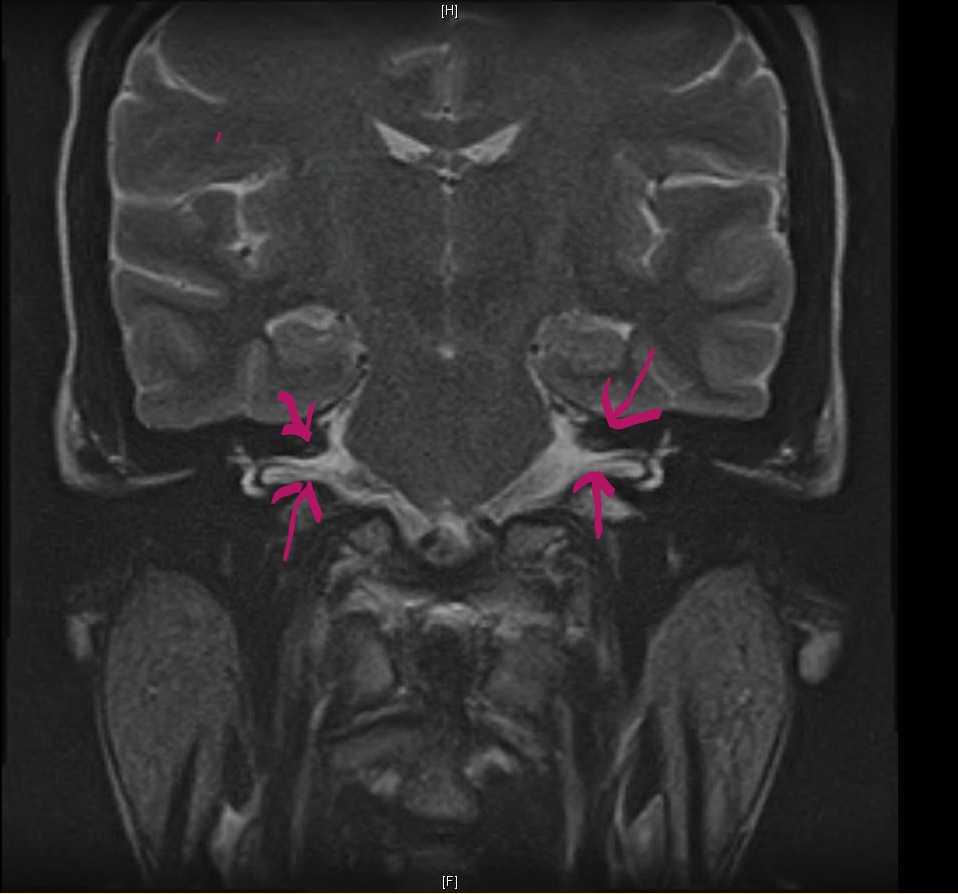
Case Presentation: 27-year-old African American woman with no medical history presented with one day of sudden onset bilateral hearing loss and tinnitus. Review of systems was positive for red eyes, blurred vision, photophobia and gait imbalance. This constellation of symptoms was preceded by a viral upper respiratory infection. She denied excessive noise exposure, head trauma or intake of any ototoxic drugs. Vital signs were Within normal limits. Neurologic exam was significant for nystagmus and axial ataxia. Eye exam showed circum-ciliary congestion with reduced visual Acuity in both eyes (20/40). Labs were significant for leukocytosis and elevated erythrocyte sedimentation rate. Comprehensive rheumatologic and infectious work up including syphilis serology and Lumbar puncture were unrevealing. MRI of brain, orbits and Internal auditory canal was normal. Audiogram showed profound right sensorineural hearing loss and severe left sensorineural hearing loss and slit lamp findings were consistent with Iritis. A clinical diagnosis of Cogan’s syndrome was made and patient was promptly initiated on prednisone along with steroid eye drops. Within the next week her ocular symptoms completely resolved but unfortunately hearing did not improve significantly over the course of next four months as evidenced by monthly audiograms. Prednisone was gradually tapered and she was referred for cochlear implantation.
Discussion: Cogan syndrome (CS), is a rare clinical syndrome characterized by ocular inflammation and audio-vestibular symptoms with or without systemic vasculitis. Sudden onset hearing loss is the most common initial presentation (50% ). The onset is frequently preceded by a upper respiratory infecton. Diagnosis is clinical, based on a combination of ocular inflammation and audio-vestibular symptoms. No lab, immunologic or radiographic test is diagnostic of CS . Exclusion of syphilis with Treponemal Antibody testing is essential. Major contribution of radiologic tests is to exclude stroke, neoplasm and Cerebellopontine angle tumors. Formal Audiometry early in evaluation is essential to document sensorineural hearing loss and assess response to systemic steroid therapy. Systemic steroids are the main stay of treatment and probability of recovering hearing is higher if steroids are initiated early in disease course. In general Ocular and systemic manifestations are more amenable to therapy than vestibulo-auditory manifestations. Complete hearing loss eventually occurs in up-to 60% of affected cases. Cochlear Implants and hearing aids may help in cases unresponsive to steroids.
Conclusions: Cogan’s syndrome is a rare cause of sudden hearing loss in young adults and prompt initiation of steroid therapy based on strong clinical suspicion is critical. Availability of cochlear implantation has markedly altered the functional outlook for these patients.