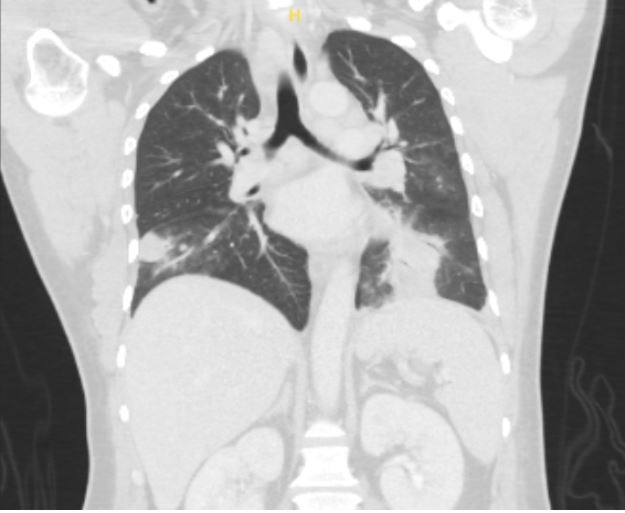
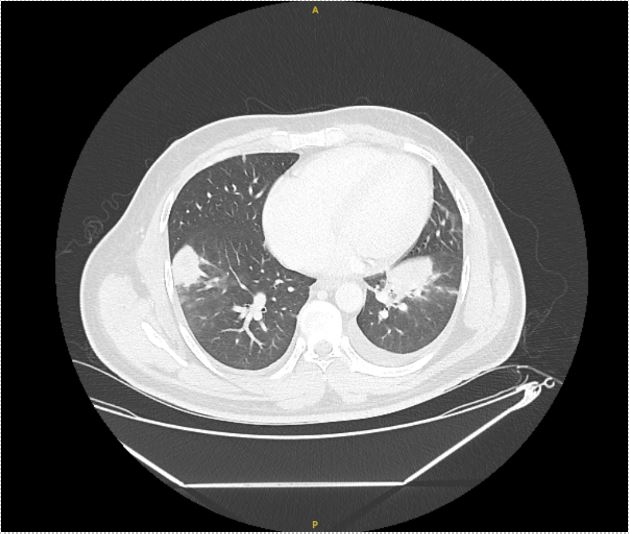
Case Presentation: A 36-year-old male with no significant medical history presented with one week of nocturnal fevers, rigors, cough associated with night sweats and 5 kg weight loss over one month. He immigrated from Guatemala 18 months ago, briefly lived in Arizona and Texas, and has worked as a landscaper locally for the past year. Review of system was negative for chest pain, shortness of breath, rashes, recent illness, or sick contacts. On admission, he had a fever of 39.4°C and was saturating 97% on room air. Physical exam was pertinent for course lung-sounds bilaterally and no skin rashes or ulcerations. Blood work was significant for leukocytosis (13.24 K/uL with neutrophilic predominance). CT Chest showed mass-like opacities in the bilateral lower lobes and left upper lobe, mediastinal and hilar lymphadenopathy, bilateral pleural effusions, and a 6mm right lung nodule (figure 1 and 2), raising concerns for neoplastic, rheumatologic, and/or infectious etiology. Our initial infectious workup, including blood and sputum cultures, HIV testing, tick-borne panel, and endemic mycoses was negative and the patient showed no improvement of symptoms or leukocytosis despite treatment with cefepime and azithromycin. On hospital day 7, bronchoscopy with lymph node biopsy was performed. Fevers persisted despite treatment with cefepime, azithromycin, and minocycline. Further infectious workup for fungal pathogens, Tuberculosis, and Coxiella was negative. Rheumatologic and oncologic workup with ANA, RF, vasculitis panel, and peripheral flow were also negative. On hospital day 14, send out testing for Tularemia IgG and IgM was positive, alongside pathology showing necrotizing granulomas positive for Francisella tularensis DNA. His antibiotic regimen was switched to IV gentamicin and PO doxycycline, leading to immediate symptom improvement on day 2 of treatment. The patient completed 10 days of targeted antibiotic therapy in-patient due to lack of insurance, with rapid resolution of fever, leukocytosis, and symptoms.
Discussion: Primary pneumonic tularemia is a rare form of tularemia that lacks the characteristic necrotizing skin lesions and lymphadenopathy of the much more common ulcero-glandular form of the disease. It has been associated with weed whacking, brush cutting, and lawnmowing, as these activities can aerosolize the pathogen from the carcass or feces of a host and infect the lungs. Given the presentation of non-specific constitutional symptoms and pulmonary findings, this presentation warrants a broad differential with an emphasis on infectious given acute onset of symptoms. Determining exposure risk was paramount for this case, but was increasingly complicated given the patient’s immigration status, recent travel through endemic regions of mycoses, and outdoor occupation with exposures to ticks and wildlife. A multi-disciplinary approach, with engagement from internal medicine, infectious disease, pulmonology, and pathology was required for timely recognition and treatment of this rare disease. Heightened awareness of this atypical presentation of tularemia will help clinicians with their differential building and avoid delay in diagnosis and treatment.
Conclusions: Diagnosing primary pneumonic tularemia requires a thorough history evaluating for exposures and effective coordination of care across multiple specialties. Early consideration, using serological or pathological testing, can hasten time to diagnosis and treatment.