Background: Accurate capture of patient severity of illness (SOI) and risk of mortality (ROM) is essential for institutional quality reporting, financial integrity, and performance on key metrics such as the Vizient Observed-to-Expected (O:E) mortality ratio. Traditional documentation relies heavily on manual provider entry and downstream Clinical Documentation Improvement (CDI) queries, creating delays, increasing administrative burden, and leaving important comorbidities under-documented. Hospitalists face additional strain due to high clinical workloads and limited time for comprehensive diagnostic coding. Efficient, automated approaches are needed to ensure accurate risk adjustment without increasing documentation effort.
Purpose: To evaluate the impact of a dynamic, algorithm-driven auto-documentation tool on the completeness of comorbidity documentation, provider workload, and key quality metrics—particularly ROM capture relevant to the Vizient mortality index.
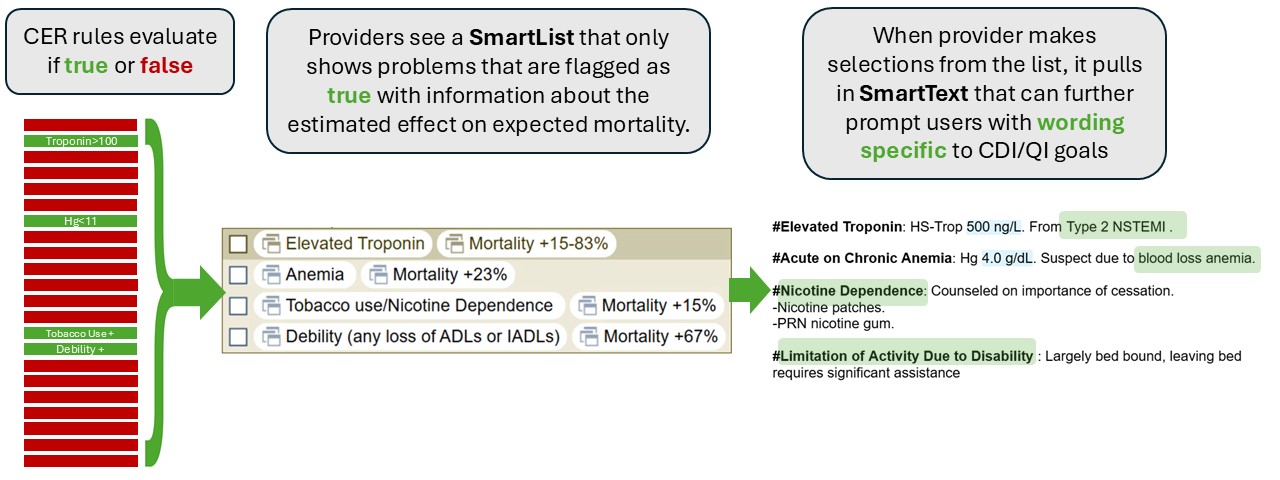
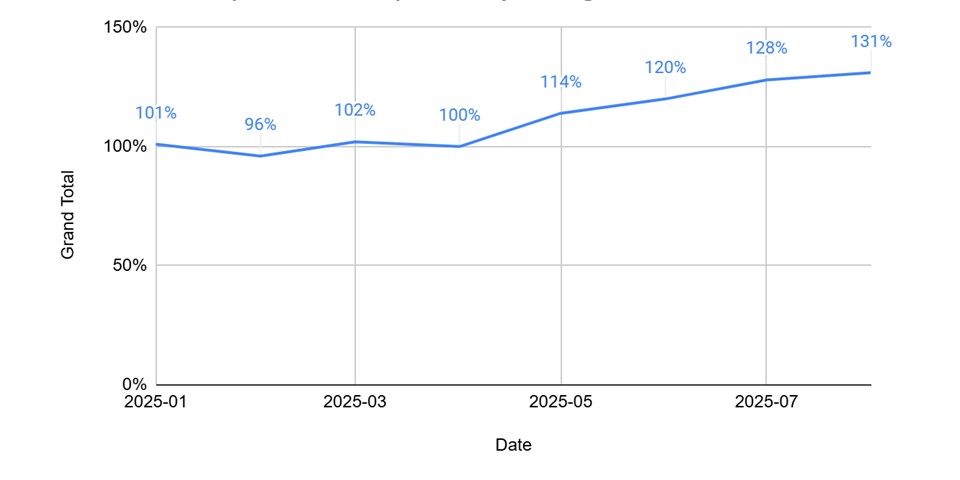
Description: UT Southwestern and Parkland Memorial Hospital collaborated to develop a dynamic auto-documentation tool embedded directly into hospitalist admission templates. The tool uses more than 40 Clinical Event Rules (CERs) built from structured patient data (laboratory values, vital signs, EKG interpretations, nursing flowsheets, and dietitian assessments) to automatically identify frequently missed but clinically significant comorbidities that influence ROM.When CER criteria are met, the corresponding comorbidity and a concise, pre-written assessment appear in a SmartList for one-click inclusion into the provider’s note. This approach eliminates the need for additional CDI queries, reduces dependence on manual chart review, and ensures consistent capture of relevant conditions. The tool can be centrally updated, allowing for real-time improvements in wording, clinical targets, and problem lists without requiring provider education or template changes.After incorporation into default admission templates (May 2025), tool utilization remained sustained with no additional rollout effort. Even though rollout was only done for the Hospitalist Division, facility-wide data demonstrated a 31% increase in the documentation and billing of our targeted problems, reflecting more complete comorbidity capture. Importantly, this improvement occurred without any increase in CDI query volume, highlighting the ability of informatics-driven automation to replace labor-intensive documentation interventions.
Conclusions: Dynamic auto-documentation using CER-driven SmartLists significantly improves comorbidity capture and enhances the accuracy of SOI/ROM representation with minimal provider burden. This innovation provides a scalable, efficient alternative to traditional CDI-dependent workflows and supports more accurate Vizient O:E mortality calculations. As documentation targets and risk-model needs evolve, centralized updating of the tool enables continuous optimization without interrupting provider workflow. This informatics-driven strategy demonstrates that targeted automation can meaningfully advance quality metrics while reducing the reliance on manual documentation processes.