Background: Manual patient-to-team assignment for Hospital Medicine (HM) at a tertiary care academic center is performed by nocturnists at the end of their shift, introducing risk for misassignment and contributing to burnout. Evidence shows standardized workflows can reduce errors by up to 25% with extrapolation to reduce medical errors.
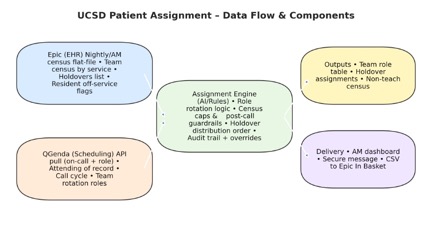
Purpose: To design and validate a prototype for an automated patient assignment engine integrated with Electronic Health Record (Epic) and scheduling software (QGenda), to reduce assignment errors and improve efficiency.
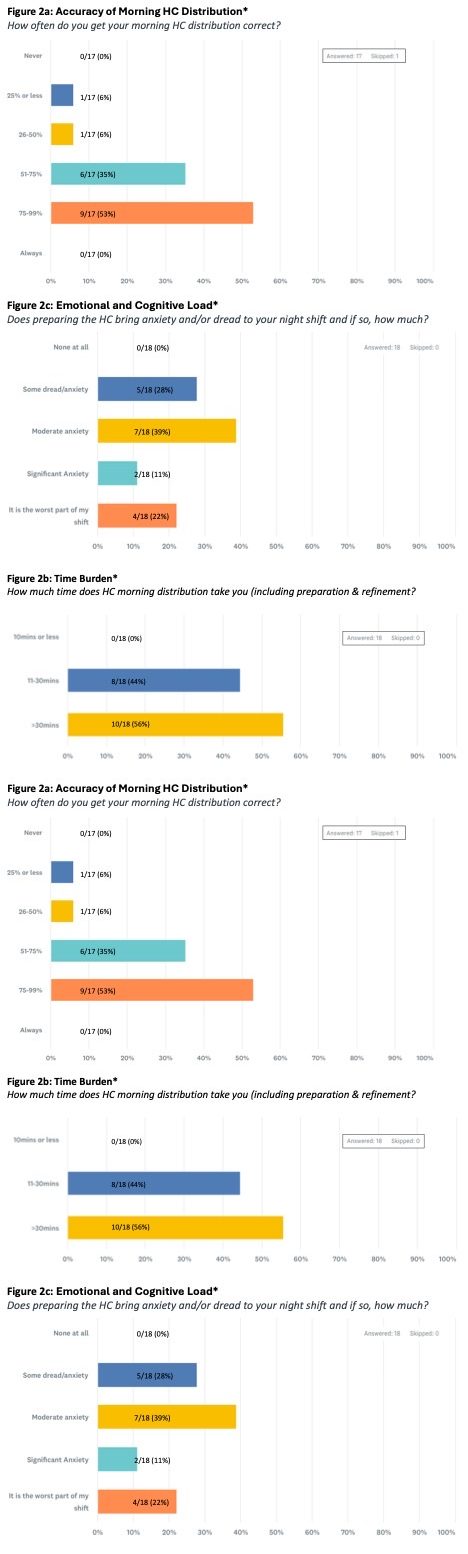
Description: A brief electronic survey was administered in SurveyMonkey to stakeholders/nocturnists’ to assess their perceptions of vulnerabilities in the morning holdover distribution process, focusing on accuracy, time burden, and clinician anxiety. The survey contained structured multiple-choice items and was distributed to all nocturnists involved in the workflow. Participation was voluntary and anonymous. Responses were collected over a defined period (6 weeks). Descriptive statistics were performed. Response rate was 86% (18/21). Baseline data showed an inconsistent, error-prone distribution process. No clinician reported perfect accuracy; 53% were correct >75% of the time, while 47% reported ≤75%, including 12% ≤50%, indicating recurrent misassignments that undermine workflow reliability.The task also carried a substantial time burden. No respondent completed it in < 10 minutes; 44% required 11–30 minutes, and 56% needed >30 minutes, highlighting marked inefficiency during the high-pressure morning period.Clinicians reported notable emotional and cognitive strain. Nearly 40% reported moderate anxiety, 33% significant anxiety or identifying patient distribution as the worst part of their shift, and only 28% reported minimal—but present—dread. No respondent reported “no anxiety.” Integrated InterpretationThe workflow was inaccurate, time-intensive, and emotionally taxing. Frequent misassignments, prolonged completion times, and high anxiety levels reveal an operationally fragile system dependent on clinician effort. Streamlining and automation offer a clear path to reducing errors, shortening task time, and improving clinician experience. An AI-driven prototype using HIPPA compliant Copilot was designed to replicate the inpatient team distribution workflow, applying constraint-aware logic to nightly Epic flat-file exports for census and holdovers. Initial development confirmed accurate replication of manual assignment logic. The next model will integrate Epic APIs for live census and holdover data and QGenda APIs for dynamic schedule, attending assignments, and rotation roles. This integration will enable continuous, constraint-driven distribution with minimal manual intervention, reducing cognitive load, and supporting scalable patient allocation.
Conclusions: The morning patient distribution process at a tertiary care academic center was inconsistent, inefficient, and emotionally burdensome. Clinicians reported less than 75% accuracy. The task consumed excessive time, often exceeding 30 minutes, and generated significant anxiety, reflecting high cognitive load and workflow fragility. Overall, the system depended heavily on clinician vigilance rather than reliable design. Streamlining through redesign, automation, or decision-support tools offers a promising path to improving accuracy, patient safety, efficiency, and clinician well-being.