Background: Transthoracic echocardiography (TTE) is a valuable diagnostic tool widely used for cardiac patients, but its accessibility and convenience have contributed to overuse. Although Appropriate Use Criteria (AUC) were developed to address this, inpatient TTE use continues to rise, with 5–8% annual increases. Studies reveal that while most TTEs meet AUC standards, fewer than one-third lead to active care changes, and 19.6% of physicians report no impact on management. This highlights the need for refined utilization practices to enhance clinical outcomes and optimize resource use.[1-2].
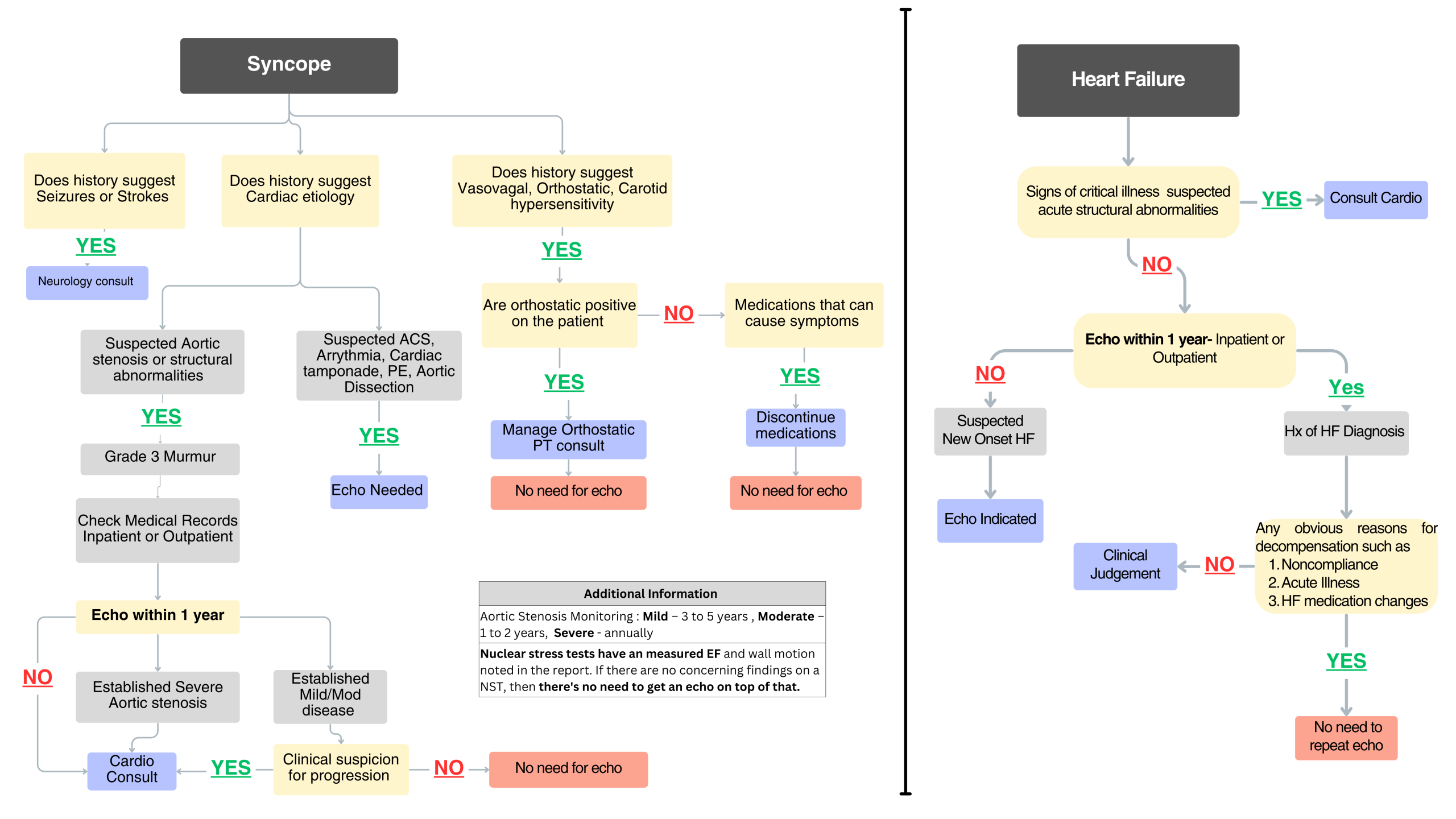
Purpose: This quality initiative aimed to reduce TTE utilization while adhering to best practices in TTE ordering in the hospital setting. A new standardized review process was created which incorporated newly drafted Syncope and CHF care algorithms, real-time dashboards to identify redundant TTEs and a tiered escalation plan when volume is higher than control.
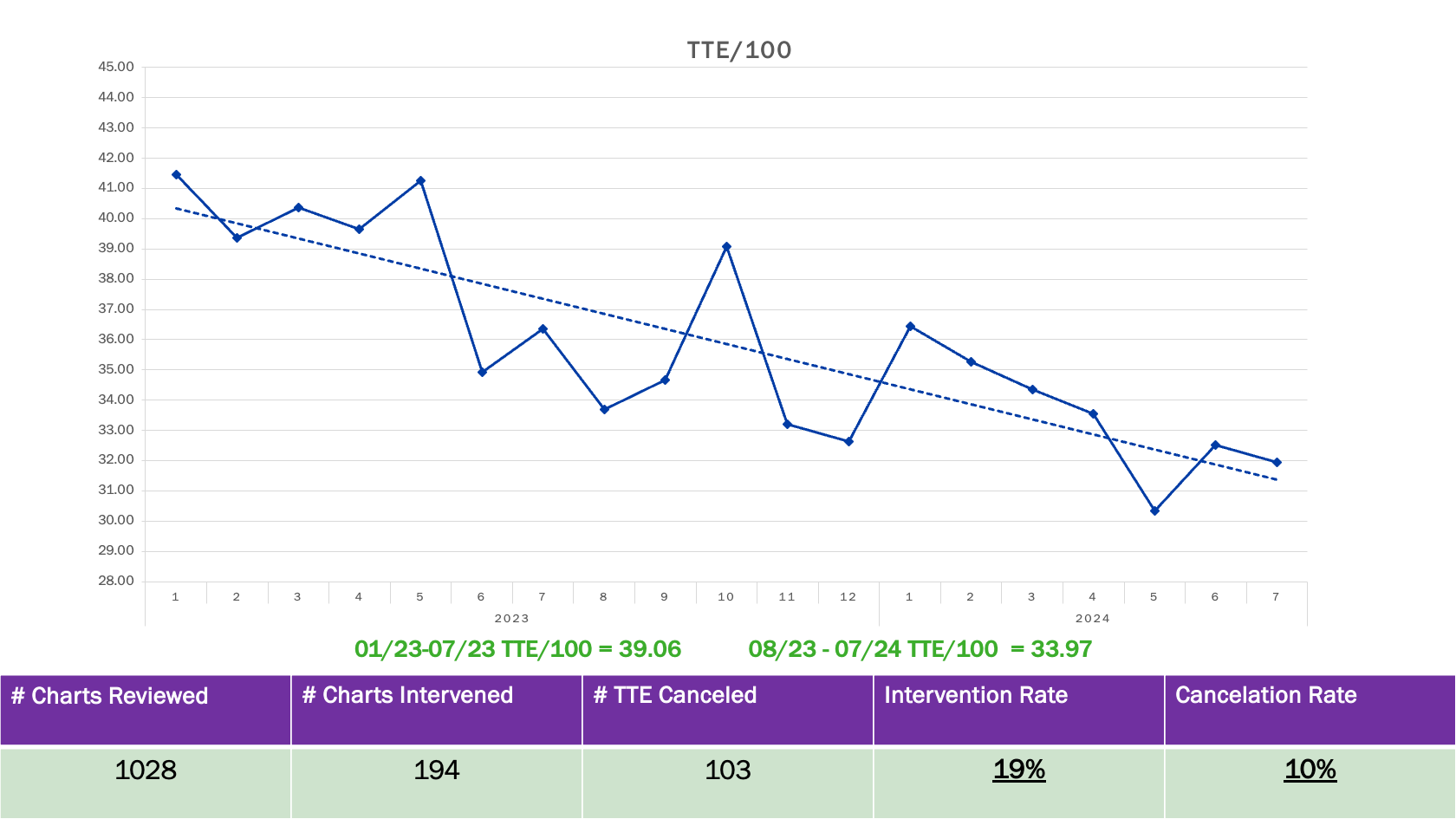
Description: To address potential overutilization adjusted to patient volume, we tracked the monthly TTE per 100 patient discharges (TTE/100). From January to July 2023, our hospital performed 5,097 TTEs averaging 39.06 TTE/100 and an average turnaround time (TAT) of 27.14 hours. We implemented a live dashboard integrated with the electronic medical record (EMR) to identify active TTE orders and flag cases with a prior TTE within the past 12 months. Additionally, we developed two targeted algorithms for syncope and heart failure—our most common indications for TTE ordering—to assist providers in ensuring appropriate utilization. Weekly chart reviews were conducted for all flagged TTE orders, with direct communication to primary teams when discrepancies were identified.From August 2023 to July 2024, we reviewed 1028 charts, flagged 194 TTE (intervention rate of 18.87%), and successfully canceled 103 TTE (cancellation rate of 10%). We noticed a reduction in TTE utilization from 39.06 to 33.97 TTE/100 and improved TAT from 27.14 to 25.33 hours, demonstrating the effectiveness of our diagnostic stewardship initiative.
Conclusions: This diagnostic stewardship initiative not only reduced TTE utilization and improved TAT, we also fostered a positive culture change within the hospitalist team. Since the project’s launch, providers demonstrated increased diligence in documenting the clinical indications for TTEs, routinely reviewing outpatient and prior echocardiograms, and ensuring that new orders aligned with clinical needs. Hospitalists and residents often appreciated being informed about active TTE orders, especially in cases where they were unaware an echocardiogram had been ordered. These changes reflect improved communication, enhanced awareness of resource use, and a collaborative effort to optimize patient care without adding significant burdens to provider workflows.