
Background:
Medication misuse was underscored in 1999 when the Institute of Medicine (IOM) recommended that reduction in medication errors be considered a national priority. IOM has emphasized the need to improve health care by adopting a team approach to patient care. New drug entities and increasingly complex regimens drive up health care costs and raise the likelihood of misuse of medications. Pharmacists have long played an important role in decreasing medication misuse by collaborating with physicians in drug therapy. There have been studies demonstrating that pharmacists' recommendations can prevent adverse drug events and medication errors. Other studies have demonstrated the decreased cost of therapy and improved outcomes with the involvement of a clinical pharmacist.
Methods:
To determine the economic outcomes of a clinical pharmacist and hospitalist team managing therapy, the direct patient cost per discharge was analyzed for hospitalist teams working with and without clinical pharmacists. Direct cost instead of pharmacy cost was evaluated since clinical pharmacists may recommend more costly medications to avoid adverse drug events and decrease length of stay. The average patient severity was similar for services, and the attending physicians rotated between the services. Therefore the only difference in the teams was whether or not a clinical pharmacist was working with the hospitalist.
The clinical pharmacists that were utilized on the teams are co‐funded by a university: 55% of their salary is covered by the institution and 45% of their salary is covered by the university. This model also enhances teaching of pharmacy students and medical residents. It allows the clinical pharmacist to develop pathways and other means to streamline patient therapy.
Summary of Results:
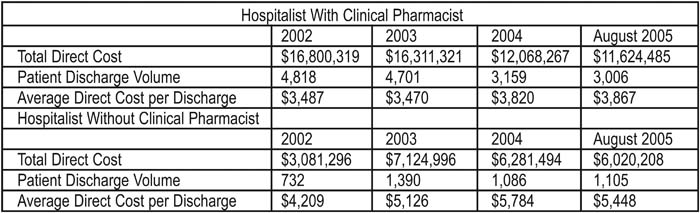
The average cost savings per discharge is approximately $1,500. Taking into account pharmacist salaries, the net savings in 2005 were $4,229,000, or $845,800 per pharmacist.
Statement of Conclusions:
A model utilizing a clinical pharmacist with a hospitalist to manage therapy for patients provides positive economic outcomes. Direct cost per discharge was utilized to determine this benefit. Our model that utilizes a co‐funded clinical pharmacist with a hospitalist shows a positive economic outcome.
Author Disclosure Block:
S. Deitelzweig, None; D.H. Lee, None; D.H. Simonson, None; E.K. Chacko, None.