Background: Over 6 million people in the US have a diagnosis of atrial fibrillation. Given the increased risk for stroke and systemic embolism, many patients are treated with direct oral anticoagulants (DOACs) to reduce their risk. In the major trials comparing to DOACs to warfarin for stroke and systemic embolism prevention in atrial fibrillation, DOACs were found to be non-inferior to warfarin for reducing stroke and systemic embolism without increasing the risk for major bleeding. However, 30-40% of patients in these DOAC trials were on concomitant aspirin therapy. To better understand the risks and benefit of dual anti-thrombotic therapy, we performed a systematic review and meta-analysis of the landmark trials comparing DOACs to warfarin in patients with non-valvular atrial fibrillation.
Methods: We systematically searched several databases from inception to October 1, 2017 for studies comparing the individual DOACs with warfarin in patients diagnosed with non-valvular atrial fibrillation. Our primary outcomes of interest were the rates of stroke/non-CNS systemic embolism (SSE) and major bleeding. The risk ratios for these two outcomes were pooled as proportions for two groups: atrial fibrillation patients on dual antithrombotic therapy (DAT) with aspirin (ASA) and DOACs and atrial fibrillation patients on DOACs but no aspirin. Sensitivity analyses were performed to verify the consistency of our results accounting for weight of each individual study to the meta-analysis.
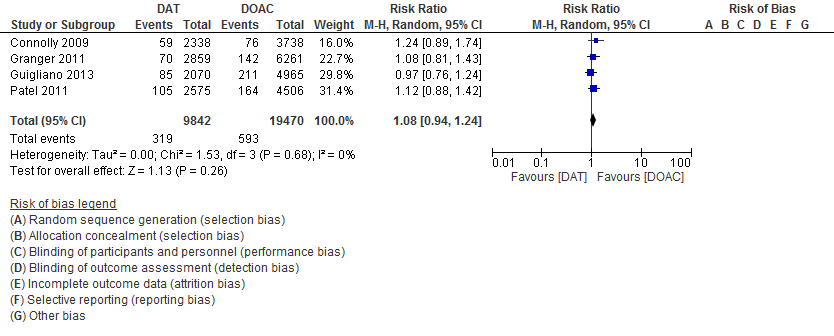
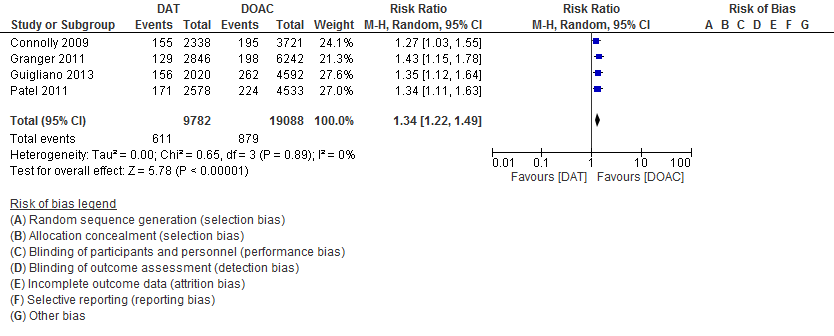
Results: Four studies with 71,683 patients were included in this meta-analysis. 19,747 atrial fibrillation patients were on combined aspirin and DOAC therapy, and 38,794 atrial fibrillation patients were on NOAC monotherapy. Compared to DOAC monotherapy, ASA use was associated with an 8% increase in SSE that was not statistically significant (RR 1.08, 95% CI 0.94 – 1.24). Compared to DOAC monotherapy, ASA use was associated with a 34% increase in major bleeding that was statistically significant (RR 1.34, 95% CI, 1.20 – 1.51). Results remained consistent after sensitivity analyses were performed.
Conclusions: Aspirin use in patients with atrial fibrillation on DOAC therapy significantly increases the risk for both SSE and major bleeding. Without evidence of coronary artery disease or acute coronary syndrome, aspirin should not be routinely used for further risk reduction against SSE in patients with non-valvular atrial fibrillation. Further trials are needed to determine if there are other subgroups of atrial fibrillation patients that benefit from dual antithrombotic therapy with aspirin and DOACs.