Background: Cardiac telemetry monitoring in hospitalized patients is an often overused resource. In a chart review at our institution, 30% of inpatient days on general medicine services involved telemetry use outside of American Heart Association guidelines. Telemetry overuse is driven both by use outside of accepted indications and by continuing telemetry monitoring longer than clinically indicated. Changes to telemetry electronic medical record (EMR) orders, combined with training, can affect both these causes. We sought to determine if changes to telemetry orders can reduce telemetry overuse at our academic medical center.
Methods: In 2017, University of North Carolina (UNC) Hospital modified the telemetry order in its EMR. When ordering telemetry, providers were required to choose from a list of clinical indications. This list was modeled after American Heart Association (AHA) guidelines with adaptations reflecting changes in clinical practice made in consultation with the director of cardiac electrophysiology. These indications were displayed with suggested durations of monitoring. Providers were required to choose a duration of monitoring with options of 24-hours, 48-hours, and indefinite. Measures included daily telemetry census and the proportion of telemetry patients with greater than two days of telemetry. These measures were assessed in the period before and after the telemetry order change. Frequency of telemetry indication was also determined.
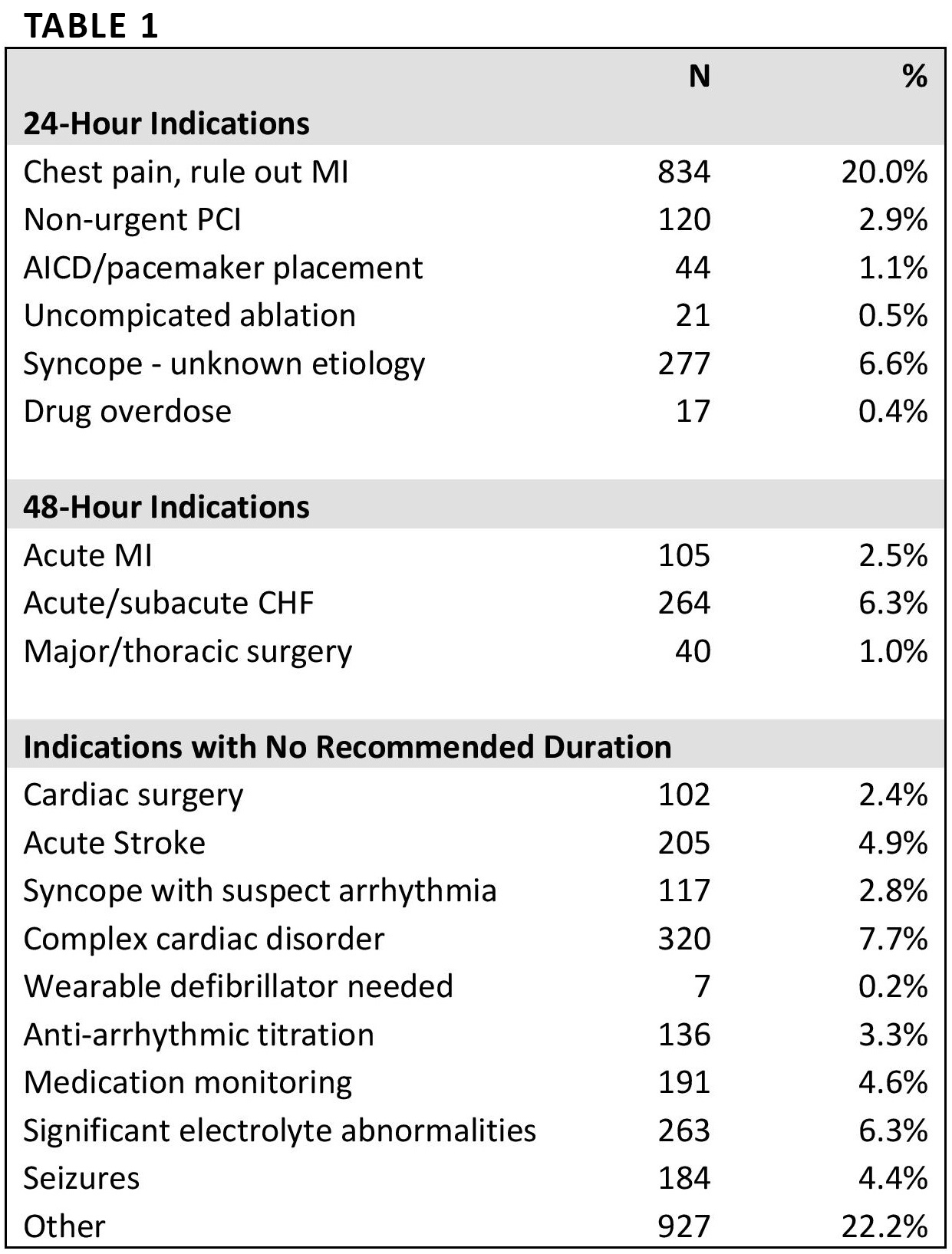
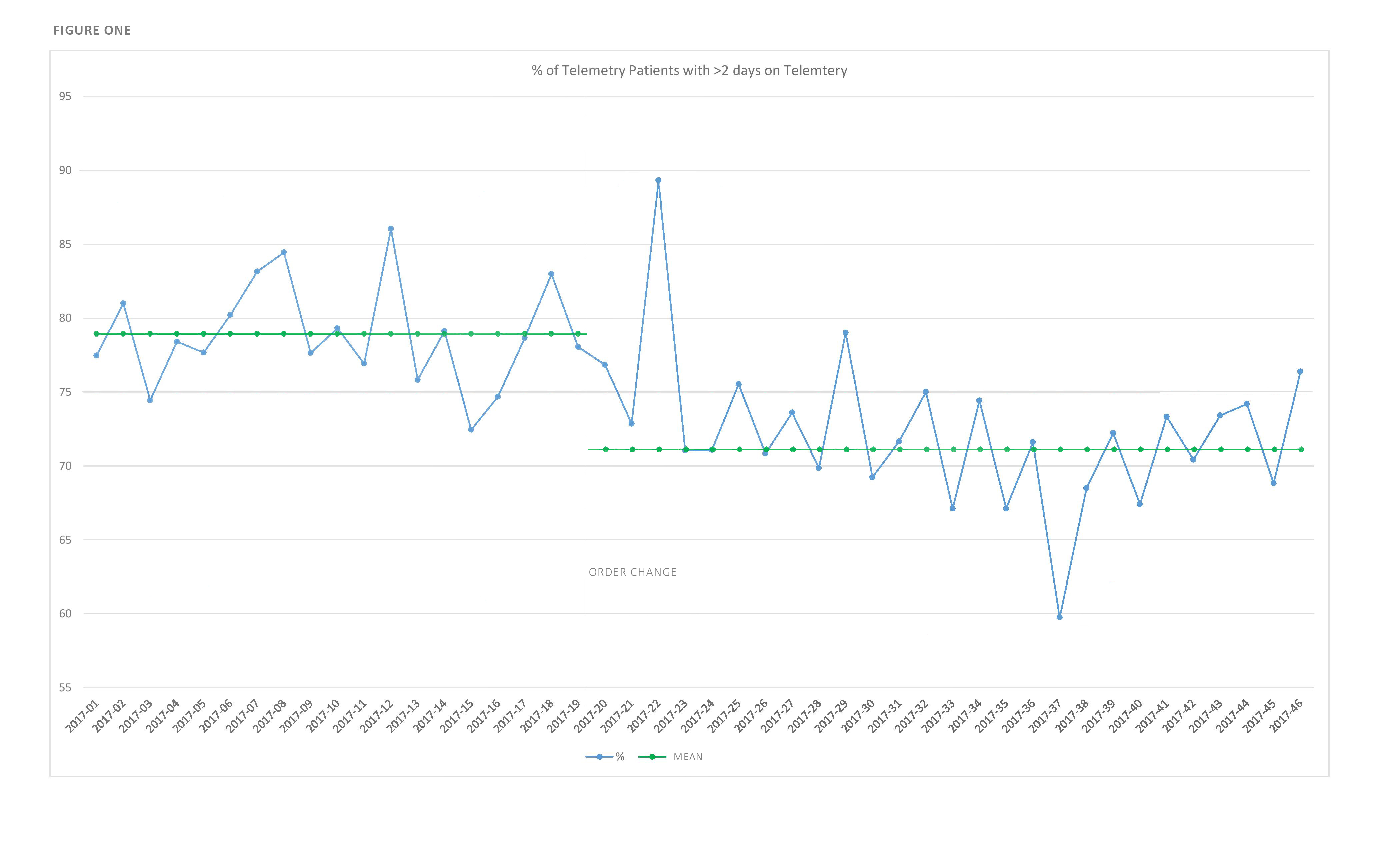
Results: In the 163 days before the telemetry order change, the mean number of patients per day on telemetry was 93.5 and, in 159 days afterwards, it was 82.1, a drop of 11.4 patients per day (12%, p-value <0.01). Of patients who were monitored on telemetry, 78.6% patients were monitored for greater than two days before the intervention and 71.3% were monitored greater than two days after the intervention (a decrease of 7.3%, p-value <0.01) (Figure 1). The leading clinical indications given for telemetry usage were “Other” (22%), “Chest Pain Rule Out MI” (20%) and “Complex Cardiac Disorder” (7%) (Table 1)
Conclusions: Incorporating the American Heart Association telemetry guidelines into telemetry orders reduced telemetry use and duration at our institution. Providers could still order telemetry outside of clinical guidelines, and directed audit and feedback could further reduce telemetry overuse. However, once implemented, EMR changes represent a low-resource intervention that can decrease telemetry usage.