Background: Atrial fibrillation (AF) is a very common condition which usually requires anticoagulation (AC). There are very clear indications of when to initiate AC but recommendations regarding bridging during elective surgery are not very clear. We here tried to answer this important question by calculating the risk of bleeding and stroke/systemic embolism (SE).
Methods: We performed a systematic search of multiple databases. Adults with AF having a CHA2DS2Vasc score of greater than 2 undergoing elective surgical procedure on AC were included. Stroke/SE was considered as the primary efficacy outcome. Major bleeding was the primary safety outcome.
Results: 108 potential articles were found after the systematic search. The full texts of 28 articles were retrieved for assessment of eligibility. 25 articles were excluded after full text review. Three articles met the inclusion criteria.
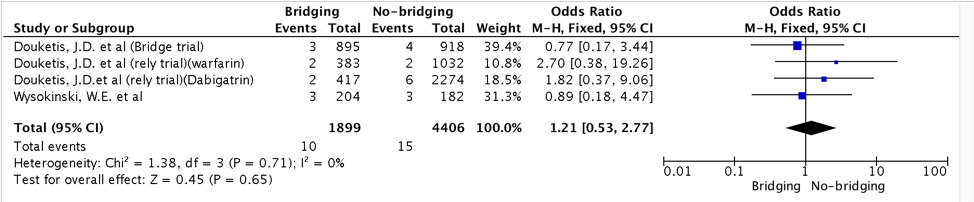
No significant difference in stroke/SE with bridging anticoagulation (risk ratio, 1.21 – 95% confidence interval [CI], 0.53 – 2.77 – Figure 1).
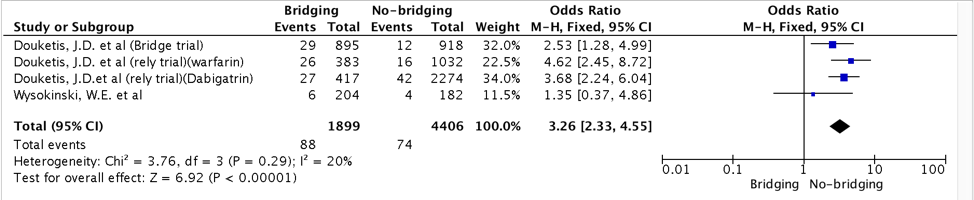
Bridging was associated with significantly higher risk of major bleeding (risk ratio, 3.26 – 95% confidence interval [CI], 2.33 – 4.55 – Figure 2).
Conclusions: Risks and benefits of bridging anticoagulation should be identified carefully. There was no significant difference in risk of stroke/SE in patients who underwent bridging but there was certainly higher risk of bleeding complications in patients who underwent bridging.