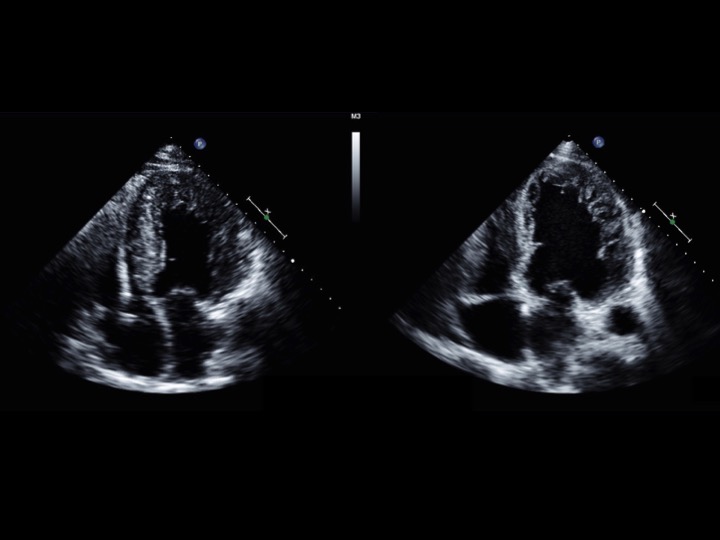
Case Presentation: A 60-year-old man with no comorbidities presented with multiple episodes of substernal chest pressure and reduced exercise tolerance. Cardiac catheterization was notable for severe systolic dysfunction with left ventricular dilatation without coronary disease. Echocardiography was significant for an ejection fraction (EF) of 20% with global hypokinesis and extensive left ventricular (LV) trabeculations consistentwith non-compaction. Repeat echocardiography after nine months of optimal medical therapy for systolic heart failure did not yield any significant change in EF, degree or depth of visible trabeculations, or LV cavity size (LV diameter, end diastole [LVIDd] 7.5cm, LV mass index 197 g/m 2 ). At this time, the patient met indications for cardiac resynchronization therapy (CRT), with QRS prolongation and presence of left bundle branch block (LBBB) morphology on his electrocardiogram (ECG), and underwent implantation of a biventricular ICD. On repeat visits, he improved clinically, with reported increased exercise tolerance. Echocardiography two years after initiation of CRT revealed an EF of 35%, decreased LV cavity size (LVIDd 5.3 cm, LV mass index 143 g/m 2 ), and notably decreased LV trabeculations.
Discussion: Left ventricular non-compaction syndrome is a frequently undiagnosed cardiomyopathy that has myriad clinical manifestations; as many as 9% of all clinically apparent cardiomyopathies may fall under this category. Heart failure in the setting of non-compaction cardiomyopathy represents a therapeutic dilemma. Current guidelines recommend treating such individuals with established pharmacologic therapies for systolic dysfunction, such as beta-adrenergic blockade and ACE inhibitor therapy. However, it is unclear if subjects with non-compaction are capable of responding to these therapies, as in the case we have presented. A few observational studies have noted some response, particularly in systolic function and functional capacity, to CRT, as well as structural remodeling and reversal of trabeculations in the myocardium.
Conclusions: To date, there are few treatment strategies that exist for left ventricular non-compaction, aside from pharmacologic and interventional therapies for systolic dysfunction. Cases such as ours suggest that CRT has a role in inducing improvement in cardiac function, morphology, and exercise tolerance.