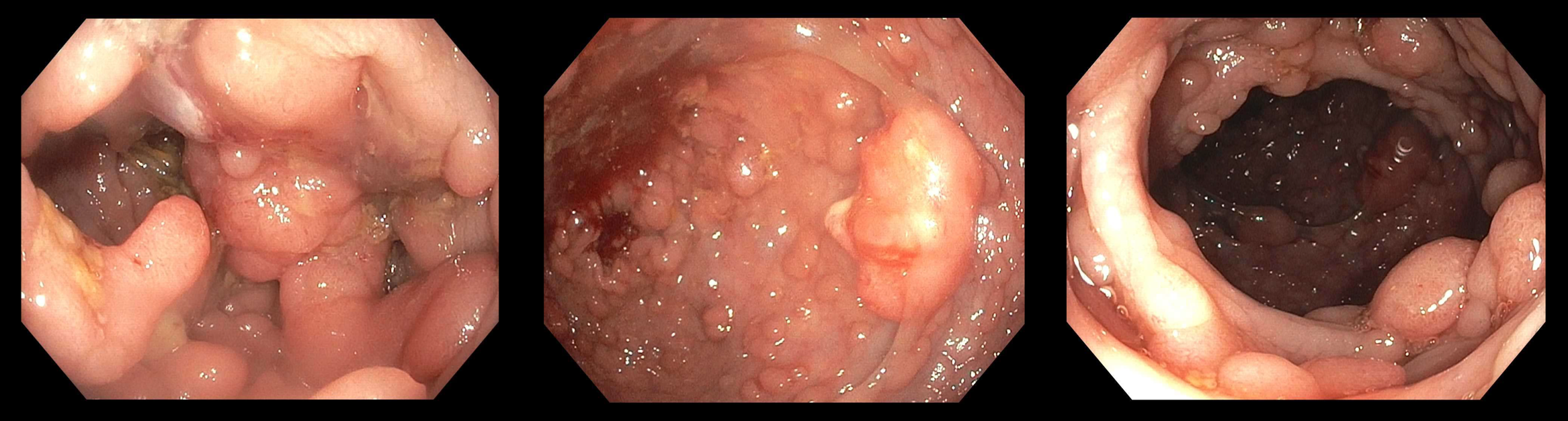
Case Presentation: We are reporting the case of a 25-year-old Hispanic gentleman with a strong family history of Familial Adenomatous Polyposis (FAP) and Colorectal Cancer (CRC) who presented for evaluation of abdominal pain, recurrent bloody stools, and profound weight loss. Initial Hb was 7.2 g/dL, and abdominal examination showed generalized rigidity and tenderness worse in the left lower quadrant. Colonoscopy revealed multiple large, non-bleeding polyps in the entire colon and up to the dentate line. The pathology report was positive for tubulovillous adenoma. The patient underwent an emergency laparoscopic-assisted proctocolectomy with Brooke ileostomy. The surgical pathology report showed grade 2 moderately differentiated adenocarcinoma. Immunohistochemical stains were positive for the expression of MLH1, PMS2, MSH2, and MSH6 mismatch repair proteins. His hospital course was uneventful, and he was discharged home to follow up with medical oncology, surgery, and primary care.
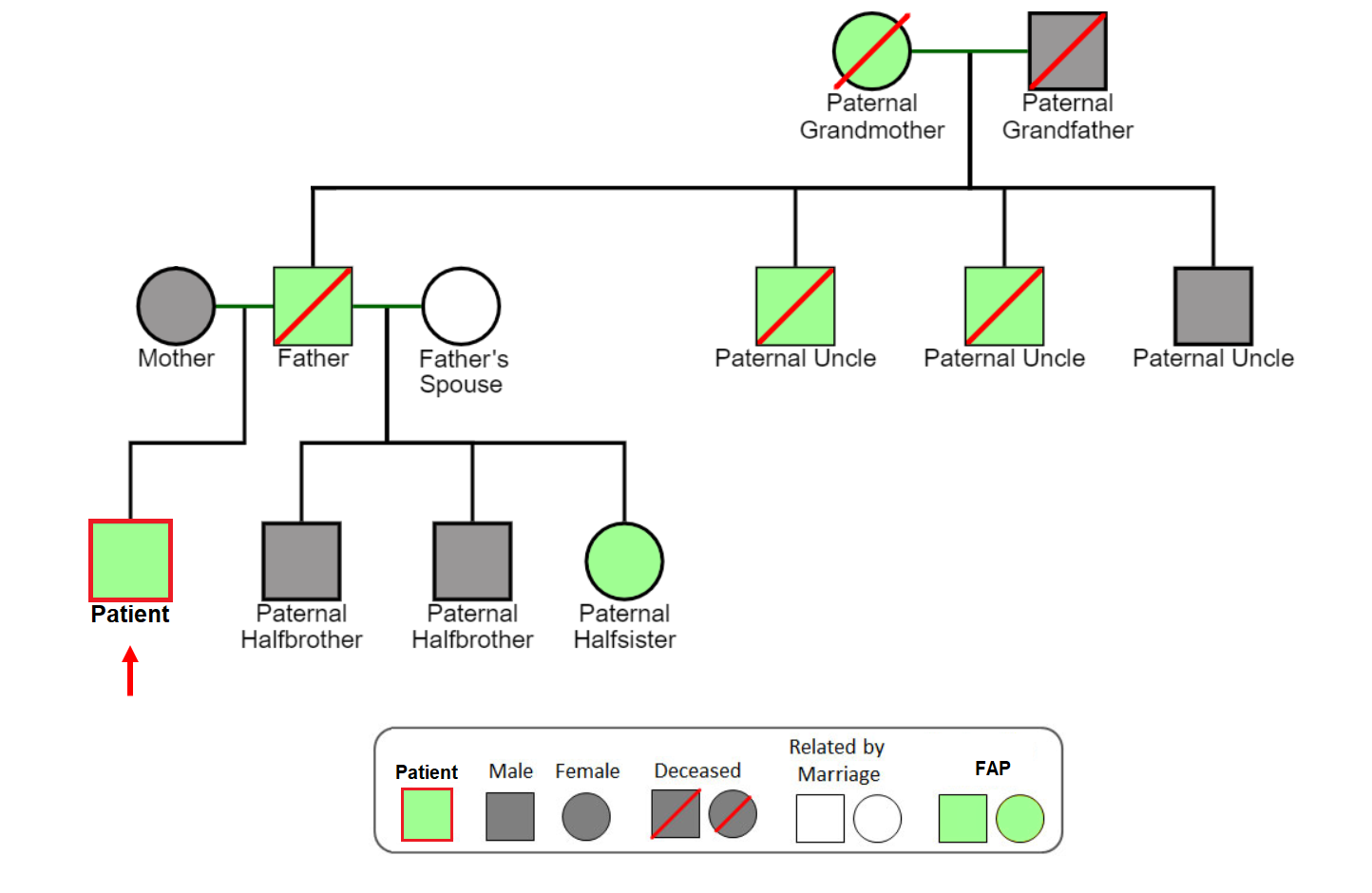
Discussion: FAP is a rare genetic disorder classically inherited in an autosomal dominant pattern, which affects about 1 in 8 300 individuals (1). The Hispanic population has limited data regarding the spectrum of FAP mutation and clinical manifestation. However, there is significant anecdotal evidence that the prevalence might be higher, with one only known Hispanic familial cancer registry in Puerto Rico (2). The development of FAP involves the germline mutation of adenomatous polyposis coli (APC) gene on chromosome 5 (3,4). The surgical pathology examination in our patient showed Grade 2 moderately differentiated adenocarcinoma with mismatch repair proteins, as mentioned above. Our patient’s father was diagnosed with CRC and later died from complications of the disease at 34. His half-sister had colon resection for CRC at the age of 17. Also, his paternal grandmother, uncles, and siblings were diagnosed in their teens. The patient is an undocumented immigrant who lives below the poverty line and without health insurance. Similarly, his family members were previously diagnosed, and unfortunately, none of them were able to consult a medical geneticist. Further highlighting the difficulties of his social situation and health illiteracy is the fact that during his childhood, his painless bleeding had been wrongly attributed to constipation. This was a challenging case because of the emergency surgical resection in a patient with extensive family history without previous counseling, who was hospitalized with complications from lower GI bleeding due to FAP and CRC. This case brings to the fore the importance of health education and access to basic healthcare, especially in minority populations in underserved communities (4,5).
Conclusions: To reduce the associated healthcare costs and morbidity and mortality of cancer in general, especially those with associated strong risk factors such as FAP and CRC, early genetic counseling, timely screening, appropriate risk-reducing medical and surgical interventions, and regular lifetime follow-up of index cases are crucial. It is also imperative to promote health literacy, especially in communities with low socio-economic status who are often at a disadvantage. Lastly, there is a need for continued research on FAP, especially in minority populations, with increased promotion and use of familial cancer registries to reduce the overall burden.