Case Presentation: 57-year-old woman with reflux disease, hypertension and obesity presented with scleral icterus and abnormal liver enzymes two months after starting compounded Tirzepatide. Her baseline hepatic function panel was normal, but after five injections of Tirzepatide her AST/ALT was noted to be elevated to 509/619 U/L. Viral hepatitis panel was negative; workup showed positive ANA. Her ferritin was 516 ng/ml, with mild alpha-1 antitrypsin elevation but work up otherwise was unremarkable. Despite discontinuation of Tirzepatide her liver function worsened, prompting admission. Initial labs showed AST 1859, ALT 1765, bilirubin 6.9, ALP 297, INR 1.9. She was managed conservatively in hospital and her transaminases improved without intervention, but cholestasis progressed (bilirubin 12.9, ALP 303, INR 2.1). Liver biopsy revealed hepatocellular dropout with mixed infiltrate and bile duct injury, consistent with DILI. She was discharged with stable enzymes. But within a few days she was readmitted with nausea and jaundice. Her labs showed AST 1405, ALT 1136, bilirubin 14.8, ALP 330, INR 2.4. Corticosteroids were started for suspected autoimmune-mediated DILI. AST/ALT improved, but cholestasis and coagulopathy worsened (bilirubin 16.7, INR 2.8). By day 5 of steroids, she developed grade 2 hepatic encephalopathy which progressed. With acute liver failure she met criteria for Status 1A transplant listing and underwent orthotopic liver transplantation within 36 hours. Explant pathology showed chronic inflammation with lymphocytic infiltrates, plasma cells, bile ductular proliferation, centrilobular necrosis, and bridging fibrosis without malignancy suggestive of progressive liver injury.
Discussion: GLP-1 receptor agonists (GLP-1 RAs) have experienced a rapid rise in the United States due to their demonstrated efficacy in glycemic control and weight loss. While common gastrointestinal side effects—such as nausea, vomiting, diarrhea, and constipation—are well-documented, more serious adverse events, including pancreatitis and bowel obstruction have also been reported. In contrast, hepatotoxicity remains a rare and underrecognized complication, particularly in the context of both FDA-approved and compounded formulations. This case presents a striking instance of progressive acute liver failure in a patient using a compounded GLP-1/GIP receptor agonist—specifically, compounded Tirzepatide—for weight loss. The severity of liver injury in this patient underscores a potential risk that may be heightened with compounded products, which can vary in quality and formulation standards. Although GLP-1/GIP receptor agonists are generally considered safe, this case highlights the importance of clinical vigilance regarding potential hepatotoxicity.
Conclusions: This case highlights a rare but serious adverse effect of GLP-1 receptor agonists, underscoring the need for heightened vigilance as their use continues to rise. Clinicians must remain alert to potential hepatotoxicity, particularly with agents like Tirzepatide, and recognize early signs of drug-induced liver injury. Regular laboratory monitoring and proactive follow-up are essential to ensure patient safety. Ultimately, physicians should maintain a low threshold for discontinuing therapy when liver injury is suspected, prioritizing patient well-being over therapeutic continuation.
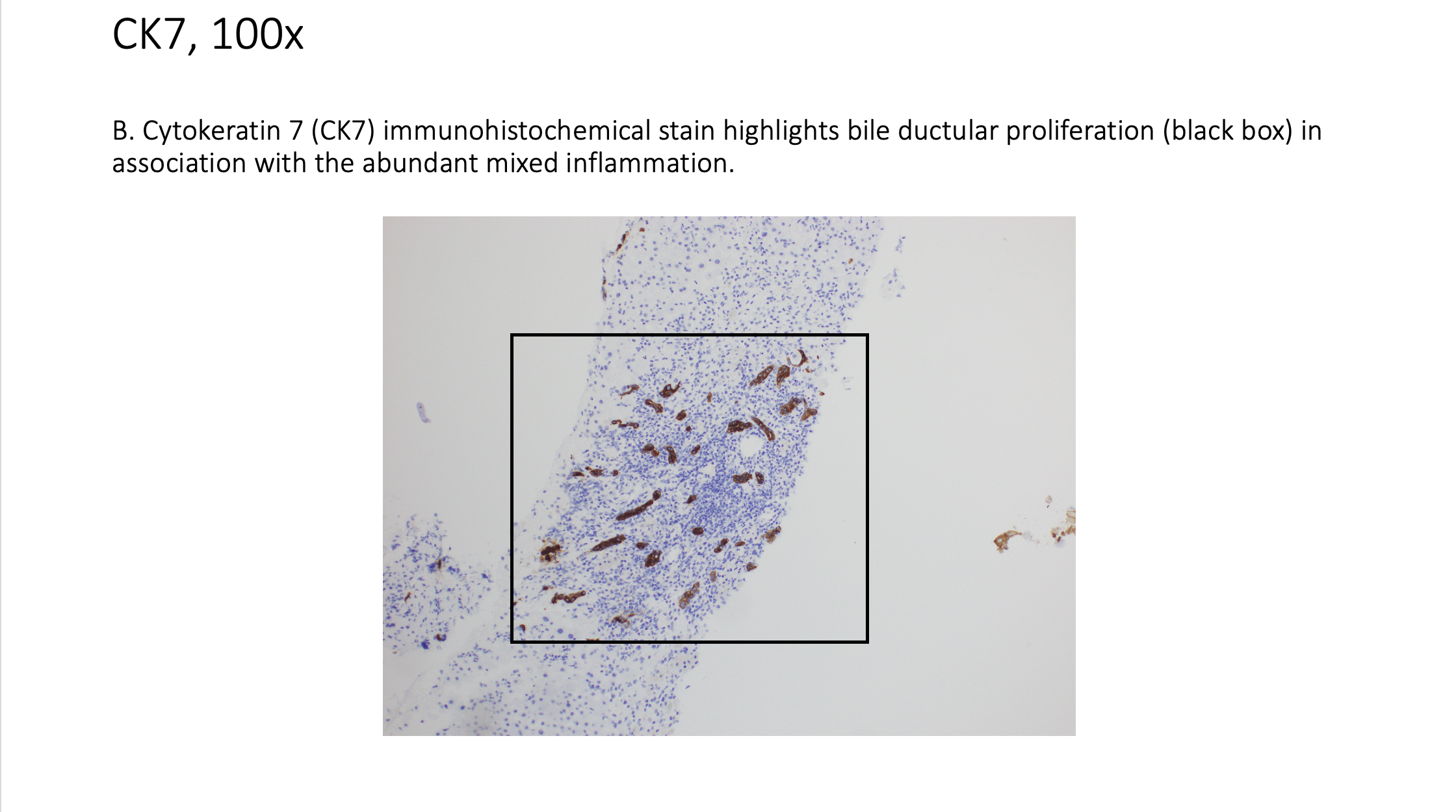
.png)