Background: As of March 30, 2022, the Food and Drug Administration now recommends follow up thyroid function testing (TFT) for children less than 4 years of age who have received IV iodinated contrast for imaging or procedures within 3 weeks of receiving contrast dye due to recent studies reporting subsequent thyroid dysfunction and the potential for future cognitive and developmental disabilities. Frameworks that ensure routine laboratory follow up in a small cohort of patients who are not easily identified by a particular diagnosis have not been well studied. Multi-faceted solutions are needed for cross-encounter providers to identify the patient as at-risk for thyroid dysfunction, to recall the timing and tests needed, to interpret the results, and to communicate this information to both primary care providers (PCP) and caregivers. We aimed to increase compliance with checking TFTs or communicating the need for TFTs to be checked to the PCP in patients 0-3 years old who had an iodinated contrast study on/after March 30, 2022 by 20% in 3 months and by 75% within 12 months.
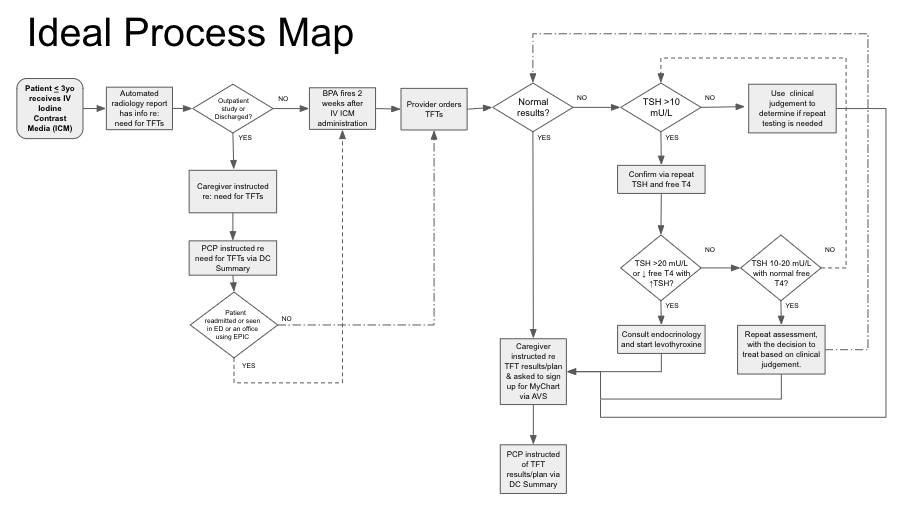
Methods: Stakeholders were gathered. Primary drivers of success were identified and the process was mapped out in detail across encounters to identify opportunities and barriers. Measures included percent of at-risk patients for whom there was communication regarding the need for TFTs with PCPs via discharge summary, caregivers via after visit summary (AVS), and TFTs completed within the recommended timeframe. We leveraged EMR tools including a best practice advisory (BPA), conditional SmartText in inpatient discharge summaries, and conditional automated information on radiology results and after visit summaries to both identify at-risk patients and improve cross-encounter communication between providers and the extended care team. The Model for Improvement was utilized testing changes through PDSA cycles.
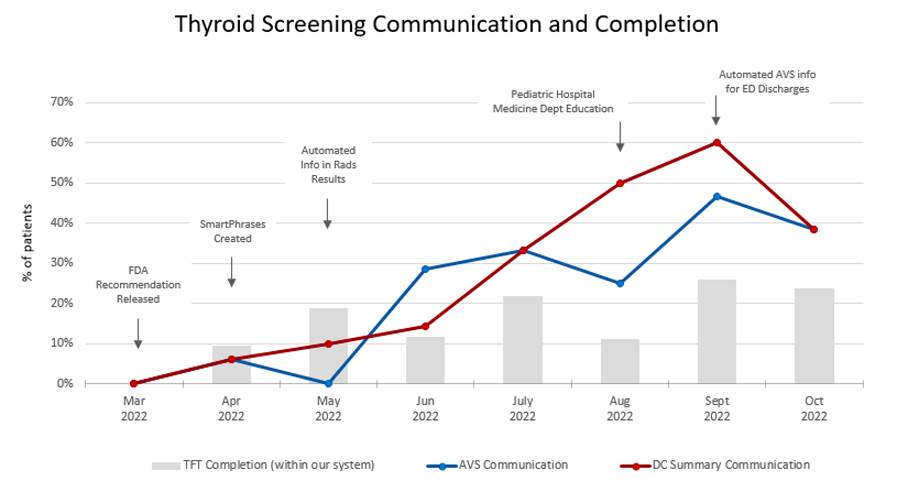
Results: Since the initiation of this project, we have identified 142 young children less than 4 years of age who received IV iodinated contrast. Of these, 39% were identified as having high-risk comorbidities (age < 3 months, very low birth weight or congenital heart disease). Compliance with communicating the need for TFTs in patients less than 4 years old who had an iodinated contrast study with PCPs through discharge summary materials increased from 0% up to 60% and with caregivers through the AVS increased from 0% up to 47% in 6 months. Since implementation of the automated ED AVS conditional SmartText, 100% of at-risk patients discharged from the ED had information in the AVS about the need for TFTs. The percentage of patients with TFTs completed within our system within the appropriate interval has also increased from 0% up to 26%. Of these, 29% (n=9) were abnormal or underwent further testing and/or treatment and all had high-risk comorbidities. Patients discharged from the ICU were most likely to have TFTs completed (61%), likely due to the fact that many remained admitted during the time frame in which they were due.
Conclusions: Overall, this project has been successful in achieving its aim since initiation. Our data collection is limited by the fact that only laboratory results done within our system could be reviewed for completion. We expect further improvements following the upcoming BPA and inpatient conditional SmartText implementation as these interventions will assist providers in identifying at-risk patients and streamline the process of adding this information with appropriate follow-up guidance to discharge materials.