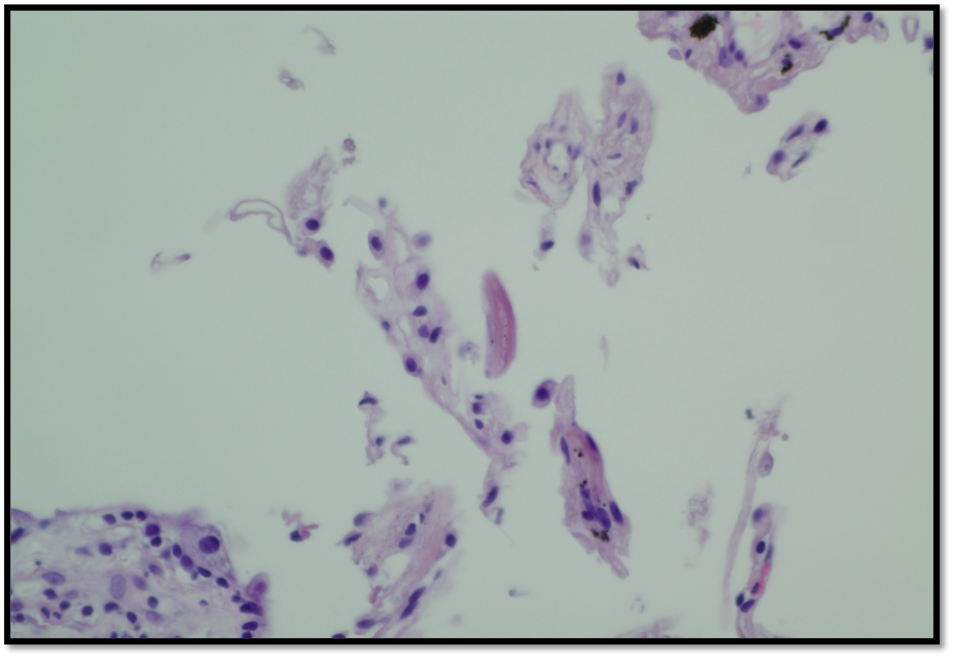
Case Presentation: An 84-year-old male veteran with prostate cancer s/p prostatectomy in 2002 with positive margins, uncontrolled type 2 diabetes, untreated hepatitis C, 50-pack-year history, presented for admission after routine labs at his primary care physician’s office revealed prominent eosinophilia of 6,900 and hyponatremia. The patient’s main complaint was generalized pruritus and a one-month pruritic rash on his back. He also had generalized malaise, weight loss and shortness of breath on exertion. He served in the United States military in Korea for a period of time during his 20s but he has not traveled internationally since then.He was seen by oncology 6 months prior and found to have markedly elevated PSA with metastatic bone lesions. The patient received 1 injection of leuprolide acetate and 3- day course of abiraterone and prednisone 5 mg prior to admission. The patient was hemodynamically stable. Physical exam was notable for catechetic appearance and diffuse, hyperpigmented maculopapular rash on the patient’s chest and upper back. Chest CT was notable for diffuse tree-in-bud opacity and nodular processes, evidence of pulmonary fibrosis and hydroureteronephrosis. Dermatology and infectious disease (ID) were consulted urgently due to concern for life-threating DRESS and systemic fungal infection, respectively. Hematology was also consulted due to concern for the hypereosinophilic syndrome. Pulmonology performed lung biopsy on hospital day 5. Skin biopsy showed spongiotic dermatitis with eosinophils. Bone marrow biopsy was unremarkable. On the 2nd day of hospitalization, ID recommended starting ivermectin daily for possible strongyloidiasis and hyperinfection syndrome. The patient’s eosinophil count started trending down on the 4th day to 5,800 after the initiation of ivermectin. On the 9th day of hospitalization, Strongyloides IgG came back positive. Stool ova and parasite testing performed twice during this admission were both negative. On hospital day 20, the result of transbronchial lung biopsy came back and showed the larval structure, which confirmed the diagnosis of systemic Strongyloides infection.The patient was discharged to a rehabilitation facility after 25 days of hospitalization with instructions to take Ivermectin 9 mg oral daily until he was seen at follow up ID appointment 10 days after discharge. His symptoms resolved and his absolute eosinophil count decreased from a peak of 9,400 to 1000 on the day of discharge.
Discussion: This case proposes a clinical dilemma about glucocorticoid administration as hypereosinophilia carries a broad differential diagnosis with overlapping and non-specific clinical manifestations. Certain rheumatologic, dermatologic and hematologic hypereosinophilic conditions are treated with the initiation of high dose glucocorticoids; especially in decompensated setting but glucocorticoids administration can also facilitate dissimilation of fungal infection such as Strongyloides in immunocompromised hosts.
Conclusions: Strongyloides stercoralis is a human pathogenic parasitic roundworm that can replicate for decades in a host without causing symptoms and in the setting of immunodeficiency may disseminate causing the potentially fatal Strongyloides systemic infection. Travel history is important even if remote. Ivermectin has a good safety and efficacy profile and should be considered early in patients with low suspicion for systematic Strongyloides infection.