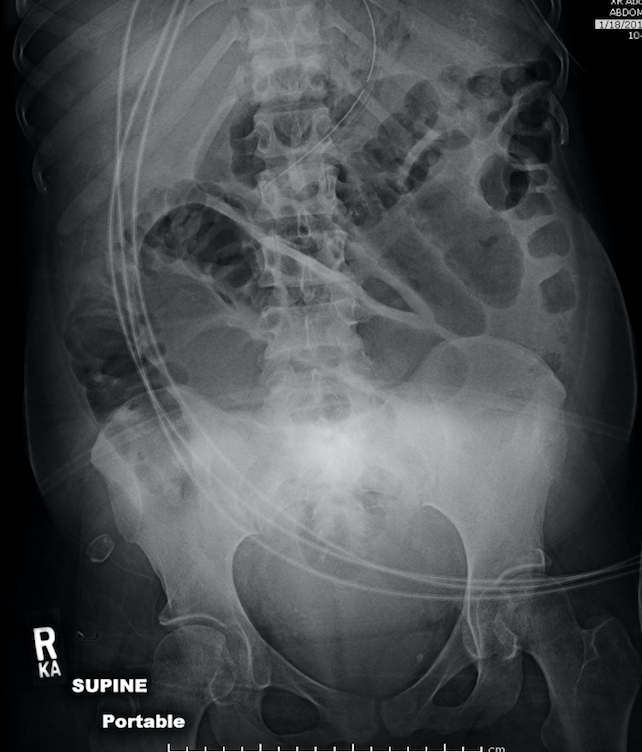
Case Presentation: A 38-year-old woman with ESRD from lupus nephritis and deceased-donor kidney transplant 6 months ago, chronic Hepatitis B, and prior tuberculosis, presented with 2 months of abdominal pain. She endorsed progressive epigastric pain, bilious emesis after meals, abdominal bloating, intermittent diarrhea, and weight loss of 30 lbs in 6 months, only tolerating a liquid diet. She had been on PD for 11 years prior to transplant. She was treated for pulmonary tuberculosis 14 years ago in South Africa for 8 months. Physical exam revealed a distended, tympanic, mildly tender abdomen; no tenderness over the transplant site; normal bowel sounds; and a small, firm peri-umbilical nodule. Abdominal CT showed a large amount of ascites and severe luminal narrowing of the small bowel, consistent with high-grade small bowel obstruction. Differential diagnosis included TB peritonitis, post-transplant lymphoproliferative disorders (PTLD), and EPS. Ascitic fluid showed 1120 WBC with 71% lymphocytes and 29% monocytes, and a SAAG of 0.8, not consistent with PTLD. Sputum and ascites MTB PCR were negative, making TB peritonitis unlikely. Peritoneal biopsy to definitively diagnose EPS and rule out TB peritonitis was deferred given high risk of adhesion and worsening obstruction, as well as concern for inadequate healing due to poor nutritional status. She was started on empiric treatment for EPS with tamoxifen and mycophenolic acid; nutritional optimization with TPN, and a diet of clear liquids as tolerated.
Discussion: EPS is a rare complication of peritoneal dialysis, with incidence of 0.7 to 13.6 per 1000 patient-years in PD. Although its pathogenesis is uncertain, the “two-hit hypothesis” theorizes that a peritoneal membrane injury from longstanding PD followed by a “second hit” leads to its development. This patient had multiple “second hit” risk factors for EPS, including long duration on PD, renal transplantation, and the use of beta-blockers and calcineurin inhibitors. Other risk factors include severe recurrent peritonitis, PD with high dialysate glucose, ultrafiltration failure, and increased solute transport. Early EPS is nonspecific, presenting with anorexia, nausea, diarrhea, and intermittent abdominal pain. Late EPS has features of ileus, peritoneal adhesions, and intermittent obstruction. EPS is diagnosed by laparotomy demonstrating a thickened, brown peritoneum enclosing the intestinal contents, although rarely done due to risks. EPS is associated with significant morbidity and high mortality of 50% at 2 years.
Conclusions: Encapsulating peritoneal sclerosis (EPS), also known as abdominal cocoon, is a rare complication of peritoneal dialysis (PD). EPS is characterized by intraperitoneal inflammation and fibrosis, causing encasement of bowel loops and a clinical syndrome of bowel obstruction. EPS should be considered in patients with a history of PD presenting with symptoms of ileus and bowel obstruction.