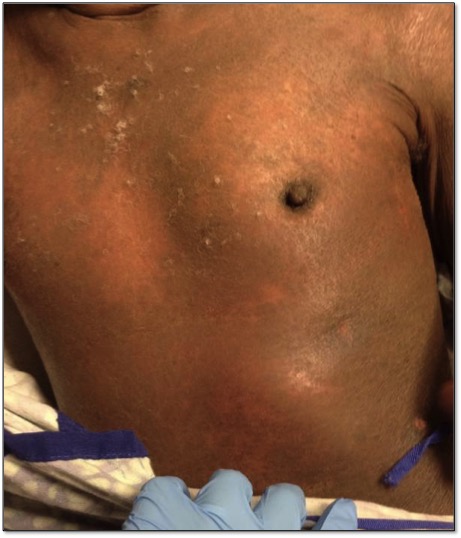
Case Presentation: A 60 yr old male with eczematous dermatitis and history of erythroderma presented to Dermatology clinic with four days of diffuse skin weeping, swelling, and bilateral lower extremity skin sloughing. Two weeks prior, he underwent partial colectomy for adenocarcinoma of his sigmoid colon. Cyclosporine was initiated for suspected erythroderma flare of eczematous dermatitis secondary to recent surgery. Physical exam was notable for diffuse xerosis and erythrodermic patches over his eighty percent of his skin. Ichthyosis and lichenification was noted over his lower extremities. Lymphadenopathy was not present.
Cyclosporine was continued on admission. Possible etiologies of his erythroderma flare included eczematous dermatitis, infection, and malignancy. Labs were significant for peripheral eosinophilia and elevated IgE. A peripheral blood smear was obtained revealing Sézary cells. Peripheral blood flow cytometry showed 3726 (62%) aberrant T cells with a CD3+, CD4+, CD7- morphology as well as a CD4:CD8 ratio of 16:28 consistent with Sézary Syndrome. The diagnosis was confirmed with PCR identification of monoclonal T-cell receptor rearrangement. Treatment initiated during the hospitalization included prednisone and photopheresis. At follow up, retinoid therapy was added to his regimen. The patient had a reduction of his Sézary cell count from 62% to 16% over three months and currently follows with Hematology and Dermatology.
Discussion: Exfoliative erythroderma is a rare condition characterized by diffuse erythema and scaling covering at least 80% of the skin surface area. The differential diagnosis for erythroderma is broad. Possible etiologies include dermatoses, infections, drug hypersensitivity reactions, systemic diseases, hematologic disorders, and malignancies such as Sézary Syndrome; an aggressive form of cutaneous T-Cell lymphoma.
The diagnosis of Sézary Syndrome is usually achieved with pathologic evaluation of skin histology, although peripheral blood evaluation may also be used. The criteria include erythroderma covering at least 80% of the body surface area, clonal T-cell receptor rearrangement by PCR or southern blot analysis, and an absolute Sézary cell count of 1000 cells/microL or one of the following two criteria: increased CD3+ or CD4+ cells with CD4:CD8 ratio >10 or, increased CD4+ cells with an abnormal phenotype (CD4+, CD7- ratio >40 percent).
Conclusions: Our patient met all aforementioned criteria and was diagnosed with T4N0M0B2 Stage IV disease. Our case is unique because his initial diagnosis came from a peripheral blood smear evaluation. Initial treatment includes topical or oral corticosteroids and retinoid therapy. Extracorporeal photopheresis is also used with a good response rate for both early and advanced-staged disease. Therefore, given the aggressive nature of his stage IV disease, photopheresis was initiated soon after diagnosis.