Background: Insulin is the preferred agent to manage hyperglycemia in the hospital. However, it is considered a high alert medication due to risk of hypoglycemia and severity of adverse events. In our institution, three hospitals currently use an order for correctional insulin based on a formula, in which the nurse calculates the dosage using the patient’s glucose. A fourth hospital uses a table-based order set, in which the dosage is already calculated based on blood glucose ranges. Current guidelines recommend standardization of insulin order sets and protocols to avoid medication errors and prefer a table-based dosing scheme. Thus, we compared the accuracy of formula-based and table-based correctional insulin dosage for the management of inpatient hyperglycemia within the Emory Healthcare System.
Methods: We collected data from the Emory Data Warehouse for all hospitalized patients that received at least one dose of insulin from a correctional insulin order, from 01/2017 to 06/2018. We compared the calculated dosage based on the formula or the ordered dose based off the table and the actual dosage administered to the patient. We defined dosing errors as: 1) over-treatment (if the dose received was higher than the ordered dose), 2) correct dose (if both doses matched), and 3) under-treatment (if the dose received was lower than the ordered dose). Manual chart review was performed for errors of greater than 10 units. Errors that were recorded as greater than 15 units were eliminated from analysis.
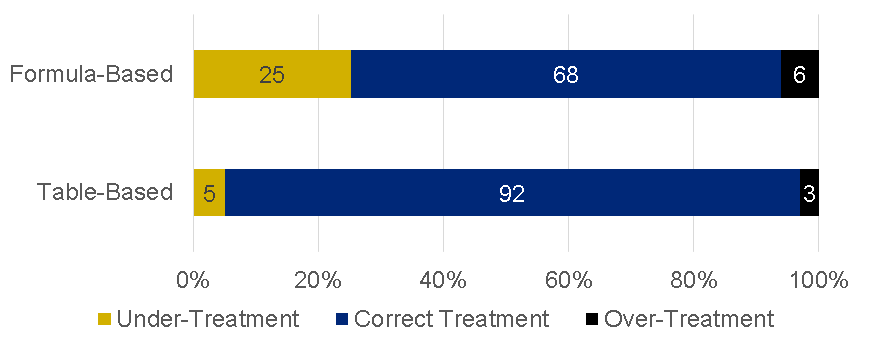
Results: Among 247,129 corrective insulin doses throughout all hospitals, 69.8% were correct, 24% indicated under-treatment, and 6.2% indicated over-treatment. When table-based dosing was used, 91.8% of doses were correct, 4.9% indicated under-treatment, and 3.2% indicated over-treatment; compared to 68.1% correct, 25.4% indicating under-treatment, and 6.5% indicating over-treatment when formula-based was used (p < 0.01).
Conclusions: One every four patients receiving a formula-based correctional insulin dose was undertreated, while one every thirty was over-treated. In our large academic health system, the use of correctional insulin is not standardized, prone to dosing errors and not meeting national standards. The used of a table-based dosing order set reduced the error rate by 24.3%.