Background: The 2016 Surviving Sepsis Campaign guidelines recommend antibiotic administration within 1 hour of emergency department (ED) presentation for patients with sepsis. While early antibiotics are associated with reduced mortality, the 1 hr policy has been criticized for its one-size-fits-all approach and risk for over-diagnosis and treatment. Clinicians and quality leaders have called, instead, for antibiotic timeliness guidelines that reflect risk of death from acute physiologic derangements.To identify more appropriate time-to-antibiotics standards, we first defined acute physiologic derangement based on four expert-recommended and readily recognizable major organ dysfunctions (MOD) and then evaluated the association between time-to-antibiotics (TTA) and inpatient mortality among sepsis patients with and without MOD.
Methods: We performed a retrospective cohort study at an academic medical center extracting data from the electronic health record (EHR) on all adults presenting to the ED between 6/1/2012 and 12/31/2016 with confirmed sepsis (change from baseline Sequential Organ Failure Assessment Score (SOFA) of ≥ 2 by 48 hours and minimum 4 antibiotic days unless death/discharge to hospice or validated sepsis discharge code). Time-stamped measurement of MOD within the first 48 hours, defined as 1) lactate ≥4, 2) Glasgow Coma Scale (GCS) ≤12, 3) shock requiring vasopressor or 4) O2 saturation/FiO2 ≤ 300, as well as antibiotic administration and inpatient mortality were collected.Multivariable logistic regression was used to evaluate association between time from ED presentation to first IV antibiotic administration and mortality with adjustment for Elixhauser comorbidity index, ED triage presence of SIRS ≥ 2 or qSOFA ≥ 2, admission year, ED volume, prior to admission location, age, sex, race and limited English proficiency.
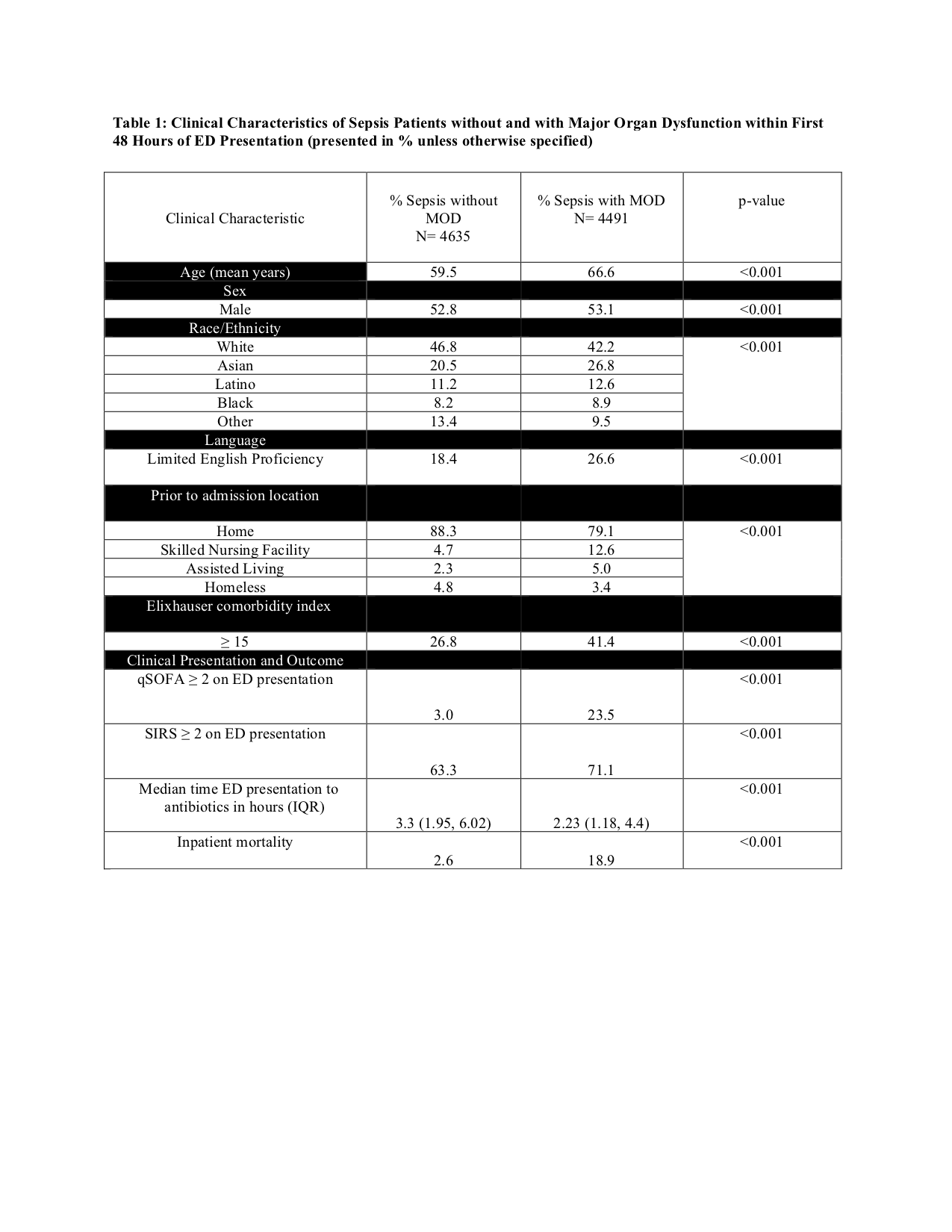
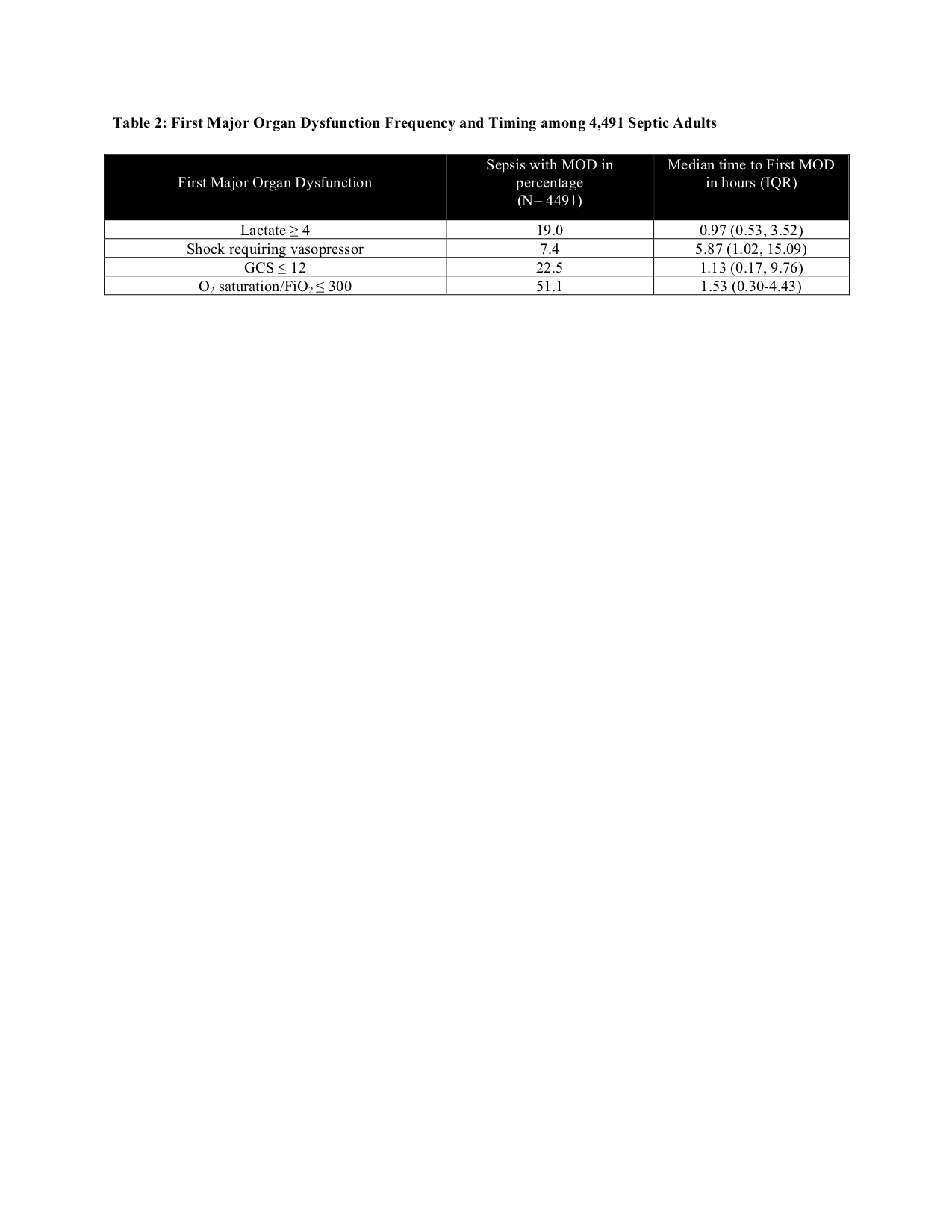
Results: There were 9,126 patients presenting to the ED with confirmed sepsis in this time period (Table 1). 4,491 (49%) patients had major organ dysfunction, and median time from presentation to MOD identification was 1.4 hours (Table 2). Median time from ED presentation to antibiotics administration was 2.3 hours v 3.7 hours among patients with and without MOD. Mortality for patients with major organ dysfunction was 18.6% (n=837/4491) versus 2.9% (n=132/4635) in those without major organ dysfunction. In all sepsis patients, there was a 2% (OR 1.02, 1.01-1.03, P=0.004) increased odds of death for every hour of antibiotic delay from ED presentation. Among sepsis patients without MOD, there was a 4% (OR 1.04, 95% CI 1.02-1.06, P=<0.001) increased odds of death, while in patients with MOD, there was a 1% (OR 1.01, 95% CI1.00-1.03, P=0.03) increased odds of death for every hour of delay from ED presentation. P-value for interaction was 0.09.
Conclusions: Delay in antibiotics and increased mortality in sepsis has previously been demonstrated, though it was hypothesized that the most severely ill patients drove this association. In this study, each hour delay in antibiotics from ED presentation increases odds of mortality in sepsis by 4% among those without MOD compared to 1% with MOD. Though patients without MOD account for fewer deaths, this difference is important for informing quality initiatives. Stratifying time-to-antibiotic targets by severity of illness, as defined by acute major organ dysfunction, could unintentionally increase the mortality of patients without early major organ dysfunction.