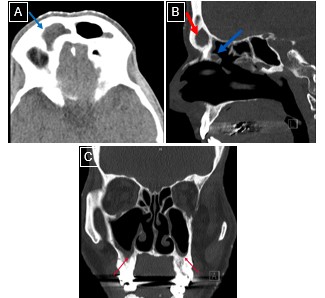
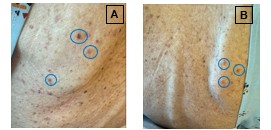
Case Presentation: A 70-year-old man with hypothyroidism and a prior clinical diagnosis of temporal arteritis (untreated with high-dose steroids) presented with several months of progressive cognitive and behavioral changes, recurrent sinusitis refractory to multiple antibiotic courses, and ~20 lbs unintentional weight loss. Over the prior 2–3 months, he developed persistent bilateral hand and foot paresthesias with electric shock-like sensations, progressive lower extremity weakness with right foot drop, gait instability causing a non-syncopal fall, and a vesicular-appearing rash on his upper back (Figure 2). He denied fevers or chills. Examination showed an emaciated appearance, marked quadriceps atrophy, diffuse weakness (most severe distally in the lower extremities), decreased distal vibration and pinprick sensation, reduced reflexes, and inability to ambulate without assistance. Labs revealed hyponatremia (Na 126 mmol/L, urine osmolality 591 mOsm/kg, urine sodium < 20 mmol/L), leukocytosis (22.3 × 10⁹/L), anemia (Hgb 11 g/dL), thrombocytosis (661 × 10⁹/L), and elevated ESR (94 mm/hr) and CRP (116 mg/L). ANA, rheumatoid factor, vitamin B12, folate, HbA1c, and Lyme serology were unremarkable. Head CT and brain MRI showed chronic pansinusitis (Figure 1); CT chest, abdomen, pelvis revealed no malignancy. Spine MRI showed an acute to subacute T11 superior endplate likely representing an insufficiency fracture, without spinal cord compression, radiculitis, or subacute combined degeneration. EMG demonstrated patchy, predominantly axonal polyradiculoneuropathy; sural nerve biopsy confirmed vasculitic neuropathy. C-ANCA and PR3 antibodies were positive, establishing granulomatosis with polyangiitis (GPA). He received pulse-dose IV methylprednisolone for three days, then a prednisone taper, and rituximab with a planned second dose in two weeks. Prophylactic sulfamethoxazole-trimethoprim and pantoprazole were started. Hyponatremia improved with sodium supplementation and nutritional support. At discharge, strength had subjectively improved, though distal sensory deficits persisted; he was discharged with outpatient physical therapy and rheumatology follow-up.
Discussion: This case highlights GPA presenting predominantly with neuropathy and chronic sinusitis, without early renal or pulmonary disease. Although vasculitic neuropathy occurs in ~19% of GPA cases, it is rarely the leading manifestation. Months of presumed bacterial sinusitis delayed recognition until neuropathy, rash, weight loss, and positive C-ANCA/PR3 clarified the diagnosis. Patchy axonal polyradiculoneuropathy with biopsy-proven vasculitis emphasizes the need to consider systemic vasculitis in unexplained multifocal neuropathy with constitutional symptoms and refractory sinus disease. Early immunosuppression can stabilize disease, though neurologic recovery may be incomplete.
Conclusions: Predominantly neuropathic GPA presentations are uncommon and may lead to diagnostic delays. Hospital clinicians should consider vasculitis in patients with progressive neuropathy and chronic sinusitis unresponsive to antibiotics and use multidisciplinary evaluation to expedite diagnosis and treatment.