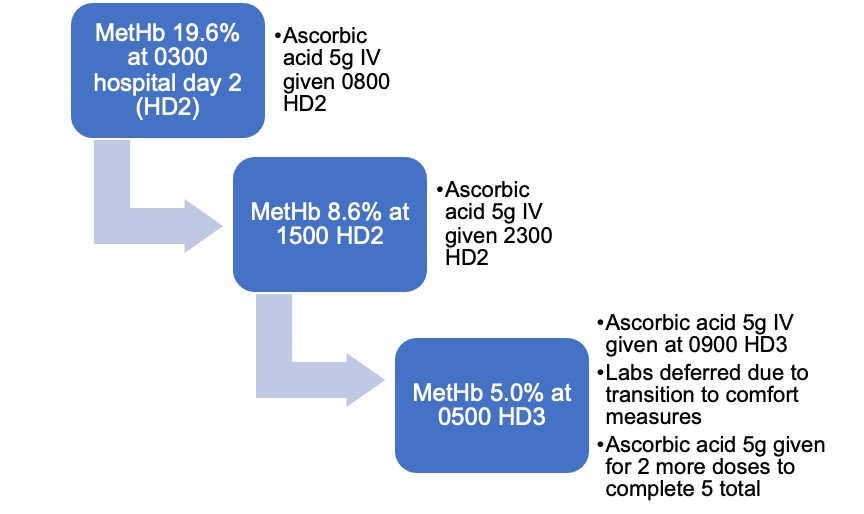
Case Presentation: A 65-year-old female with uterine carcinosarcoma was hospitalized for ascites, dyspnea, and fatigue. Initial findings revealed peritoneal carcinomatosis with massive ascites, potential liver metastases, and acute kidney injury (AKI) with creatinine 6.6 mg/dL (baseline 0.9) with oliguria. She declined dialysis. High urate (14.5 mg/dL) prompted administration of rasburicase due to an initial concern for tumor lysis syndrome. Four hours later, pulse oximetry (SpO2) was 79% on high-flow nasal cannula at FiO2 100%; arterial blood gas showed partial pressure of oxygen (PaO2) >500 mm Hg. She was lethargic but breathing was unlabored. Methemoglobin level (MetHb) was 19.6%, hemoglobin was 6.8 g/dL. She was treated with intravenous (IV) ascorbic acid (5 grams every 12 hours, adjusted for AKI) for 5 doses and one blood transfusion. Her MetHb level improved (8.6%) after one dose of ascorbic acid and again (5%) after the second, no more levels were obtained. Glucose-6-phosphate dehydrogenase (G6PD) level, resulting later, was 161 U/trillion RBCs (Normal: 127-427). While MetHb levels decreased and hypoxia resolved, her renal function, mentation and overall prognosis remained poor. After family discussions, care shifted to comfort measures and she died awaiting hospice placement.
Discussion: This patient developed methemoglobinemia secondary to rasburicase, a rare adverse effect more common in G6PD deficiency, as erythrocytes are vulnerable to oxidative damage. Reports of females suffering this phenomenon are rare. Though X-linked, females are affected by G6PD deficiency if homozygous or if heterozygous with skewed X-inactivation. The patient’s level was low-normal, but acute hemolysis and less severe deficiency may cause false-negatives. We avoided methylene blue (MB), which treats methemoglobinemia by reducing ferric iron, but worsens hemolysis in G6PD deficiency. Intravenous ascorbic acid is infrequently used at various doses to treat methemoglobinemia when MB is contraindicated. Though it acts less rapidly, it is more accessible and less toxic. Uncommon side effects of high-dose ascorbic acid include oxalate nephropathy, hypernatremia, and rare cases of paradoxical methemoglobinemia in G6PD deficiency by oxidative stress.
Conclusions: In this patient with metastatic uterine carcinosarcoma and renal failure who developed methemoglobinemia secondary to rasburicase, ascorbic acid carried minimal risk and improved hypoxia as she progressed to end-of-life care. The case highlights several important concepts. First, methemoglobinemia should be considered in hypoxic patients with discordant SpO2 and PaO2, which occurs as methemoglobin impairs pulse oximetry accuracy. Physicians should consider G6PD deficiency, even in females, when prescribing relevant medications. Lastly, when MB is contraindicated or unavailable, ascorbic acid can be used as an effective therapy for methemoglobinemia and further study should standardize dosing regimens.