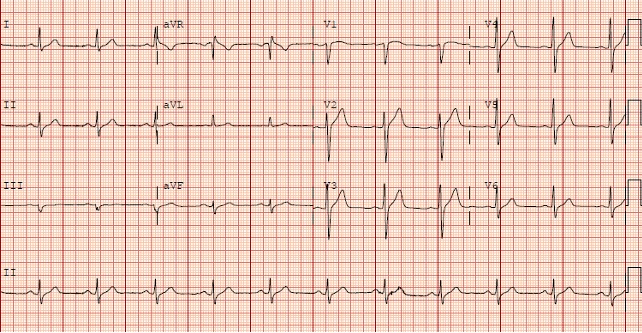
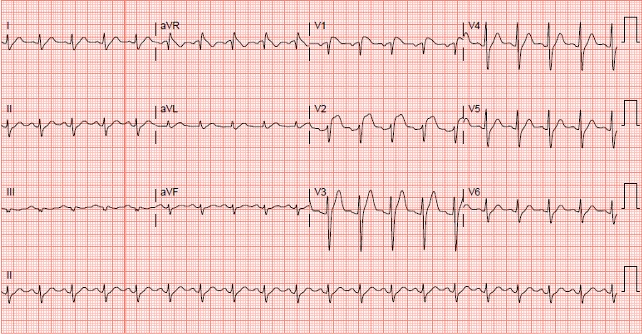
Case Presentation: 59 year old man with past medical history of renal cell carcinoma, with right nephrectomy 20 years ago, presented to the Emergency Department with fever and dysuria. Upon presentation, he was found to have a oral temperature of 102.0 F, a tender prostrate on exam and leukocytosis with neutrophilia suggestive of acute bacterial prostatitis. An EKG showed new coved ST elevations in v1 and v2 anterior chest leads which were not present in his prior EKGs. Patient denied any chest pain or pressure, shortness of breath or diaphoresis. Cardiac enzymes were negative. A POC Transthoracic echo showed normal LV wall motion and systolic function. Patient has no history of arrythmias, syncope or sudden cardiac death in family. A review of his medication history did not reveal any medication known to induce Brugada type EKG pattern. During his hospital stay, patient was treated with IV Cefepime and with resolution of fever and leukocytosis, was switched to oral antibiotics and discharged with planned outpatient follow-up to evalute resolution of EKG abnormalities and need for ICD implantation.
Discussion: Brugada syndrome is a genetic disease presenting with a characteristic electrocardiogram (EKG) and a tendency to develop malignant polymorphic ventricular arrhythmias that may lead to syncope or cardiac arrest. Spontaneous or drug-induced Type I Brugada pattern on EKG are known to increase risk of sudden cardiac death. In patients with previously diagnosed Brugada syndrome, fever is known to induce Brugada syndrome–type EKG changes and can precipitate cardiac arrest. Prognosis of fever-induced Type I Brugada pattern in asymptomatic individuals with no history of arrythmias, or sudden cardiac death in family is less well defined.
Several channelopathies involving Sodium, and less commonly calcium, channels have been identified in patients with Brugada Syndrome. Temperature dependent variation in sodium channel current was demonstrated by Dumaine et al in 1999. Thus, fever induced Brugada type EKG pattern may represent the first manifestation of Brugada Syndrome in previously undiagnosed asymptomatic individuals. However, In the absence of large scale prospective studies, the prognostic significance of fever induced Brugada pattern remains unclear. As such, the decision for further investigation with EPS/pharmacological induction of arrythmia and indication for ICD implantation remains a clinical conundrum in this sub-group of asymptomatic individuals with fever induced Type I Brugada pattern on EKG.
Conclusions: Prognostic significance of Fever – induced type I brugada pattern on EKG in asymptomatic individuals remains unclear and decision for further investigation and management for such individuals needs to be individualized on a case by case basis until further data becomes available.