Background: Mortality prediction models have the potential to improve prognostication, guide goals-of-care discussions, and support interdisciplinary care. The integration of mortality risk into clinical practice remains a subject of ongoing investigation. Several academic hospitals have recently reported promising workflows and initiatives demonstrating how predictive algorithms can support serious illness conversations and palliative care engagement(1-5). However, real-world adoption depends on clinicians’ perceptions, communication practices, and workflow integration. Our primary aim was to understand how hospitalists at a large academic medical center engaged with, interpreted, and trusted a mortality prediction model as part of their clinical decision-making.
Methods: We conducted interviews with 25 hospitalists at our institution to examine how they identify patients who may benefit from goals-of-care discussions and how they incorporate mortality prediction models into clinical decision-making. All interviews were recorded on a HIPAA-compliant platform, and transcripts were organized into an analytic matrix. Common themes were identified using a matrix-based rapid qualitative analysis approach informed by Hamilton and Finley’s rapid qualitative methodology (6), the Rigorous and Accelerated Data Reduction (RADaR) technique (7), and the Framework Method (8). Interview and field-note data were categorized across 15 analytic domains encompassing illness classification, prognostic strategies, communication styles, interdisciplinary roles, and model usability. Frameworks such as REMAP (9) and SPIKES (10) guided the interpretation of communication-related themes.
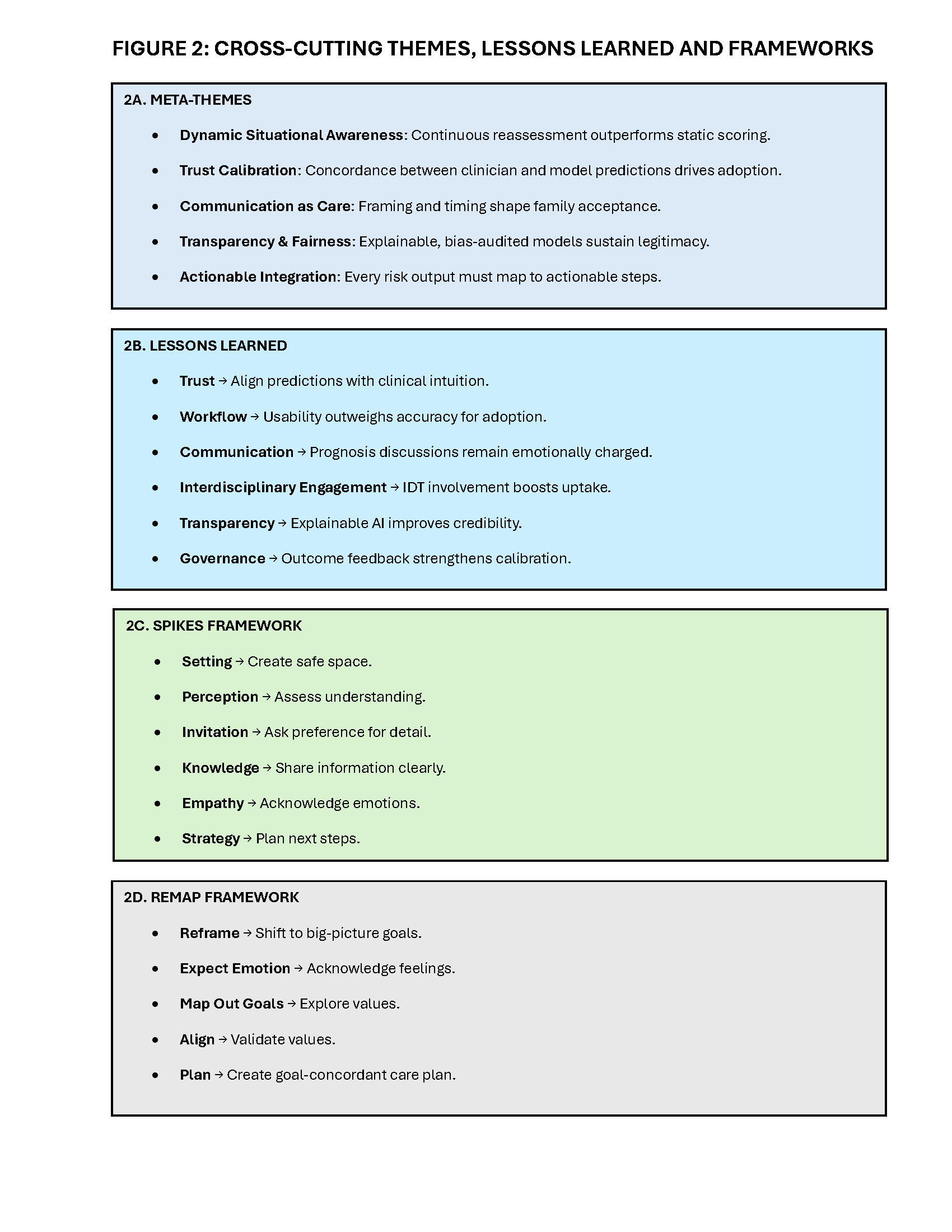
Results: Participants consistently relied on clinical severity cues that matched their intuitive reasoning. Mortality risk estimates were perceived as valuable for situational awareness, anticipatory planning, and interdisciplinary coordination. Acceptance of the model depended on concordance with bedside assessment, transparency around contributing factors, and alignment with existing workflow (Figure 1). Participants expressed a desire for greater explainability (“why this score?”), flexible notification timing, and governance strategies such as outcome feedback loops (Figure 2A). Lessons learned highlighted the importance of trust calibration, communication training, interdisciplinary engagement, and aligning risk outputs with actionable treatment pathways (Figure 2B). Communication around prognosis remained emotionally complex, and clinicians emphasized the value of structured approaches based on concepts from REMAP and SPIKES for supporting difficult conversations (Figure 2. C, D).
Conclusions: Efficient, peer-reviewed mortality prediction models can enhance clinical decision-making and communication when integrated into clinicians’ existing mental models, interdisciplinary workflows, and structured conversation frameworks. REMAP and SPIKES are effective frameworks that can be incorporated into a hospitalist’s workflow to support values-based discussions. Successful implementation of a mortality model requires transparency, usability, explainability, and alignment with patient-centered communication practices. Our findings contribute a structured roadmap for the scalable refinement of mortality prediction tools and the clinical workflows required for their effective implementation.
.png)