Background: Initial research has suggested that telehealth can provide quality care, increase efficiency, decrease cost, and potentially alleviate physician shortages in underserved communities [1]. Implementation of a telehealth service provided a significant reduction in patient length of stay with no increase in mortality rate and no decline in patient satisfaction [2]. Even with the increase in telehealth care, rural areas still experience a higher mortality rate than urban communities with the gap still widening [3]. Physician shortages in rural areas is one of the main reasons for this discrepancy. Further an estimated 21% of the US population lives in a designated rural county [4]. While telehealth has shown promise in addressing healthcare disparities in rural areas, its application in providing hospitalist services to rural post-acute inpatient rehabilitation facilities remains largely unexplored [5, 6]. Further research is needed to investigate the feasibility, effectiveness, and implementation of such models in improving access to specialized care and optimizing patient outcomes in rural post-acute settings.
Methods: Objective: To evaluate the association of transitioning to telehealth coverage and the changes in functional and general health outcomes among patients receiving inpatient rehabilitation care at Roosevelt Warm Springs Rehabilitation Hospital in Warm Springs, Georgia. Design: Retrospective descriptive cohort study.Setting: Roosevelt Warm Springs Rehabilitation Hospital, a post-acute inpatient rehabilitation facility in rural Georgia Participants: Adults discharged from inpatient rehabilitation between January 2, 2020 through December 20, 2024. Patients were categorized by period of care: pre-telehealth implementation (admitted before August 1, 2021: n = 706) and post-telehealth use (admitted after August 1, 2021; n = 1239)Intervention: Patients received standard inpatient rehabilitation; beginning August 1, 2021, medical oversight transitioned to telehealth hospitalist services. Main Outcome Measures: Primary outcomes were functional status and length of stay. Functional status was measured using Section GG self-care (range 7–42) and mobility (range 15–90) summary scores from the CMS Inpatient Rehabilitation Facility–Patient Assessment Instrument. Responsiveness was quantified using standardized response means (SRMs), calculated from admission-to-discharge change scores. Paired t-tests assessed significance of within-group change; independent t-tests compared length of stay (LOS) between periods.
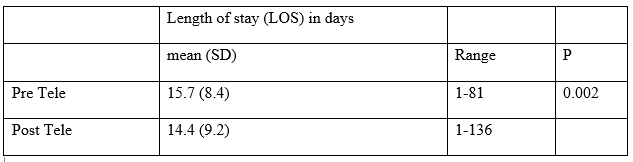
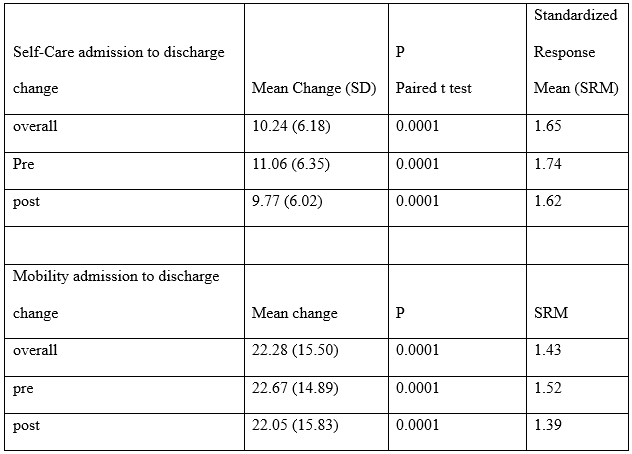
Results: Results: Most patients (79%) were discharged to an improved/home setting. Mean age at admission was 61.6 years and did not differ between groups (p=0.8). LOS was significantly shorter after implementation of telehealth services (15.7 vs. 14.4 days; p=0.002). Overall mean change (±SD) in self-care was 10.24 ± 6.18 (p< 0.0001; SRM=1.65) and in mobility was 22.28 ± 15.50 (p< 0.0001; SRM=1.43). Large SRMs (>0.8) were observed in both pre-telehealth (self-care SRM=1.74; mobility SRM=1.52) and post-telehealth groups (self-care SRM=1.62; mobility SRM=1.39).
Conclusions: The transition to telehealth hospitalist services was associated with a modest but significant reduction in length of stay without compromising functional gains. Additional research is needed to evaluate potential confounding clinical factors such as stroke severity, baseline functional status, and diagnosis to further contextualize observed improvements.