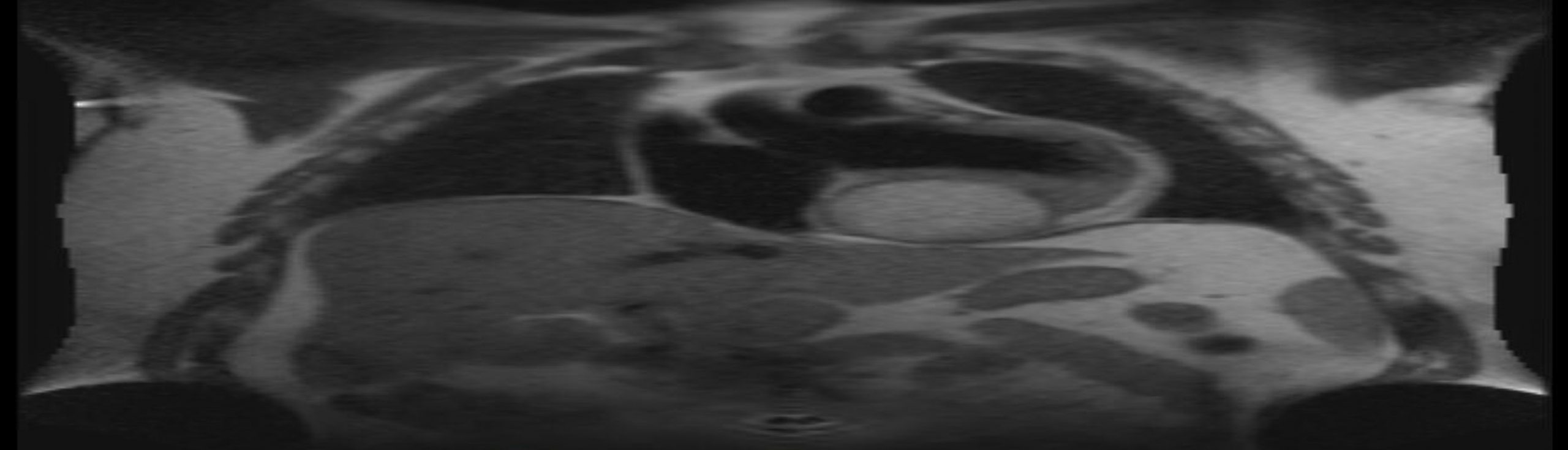
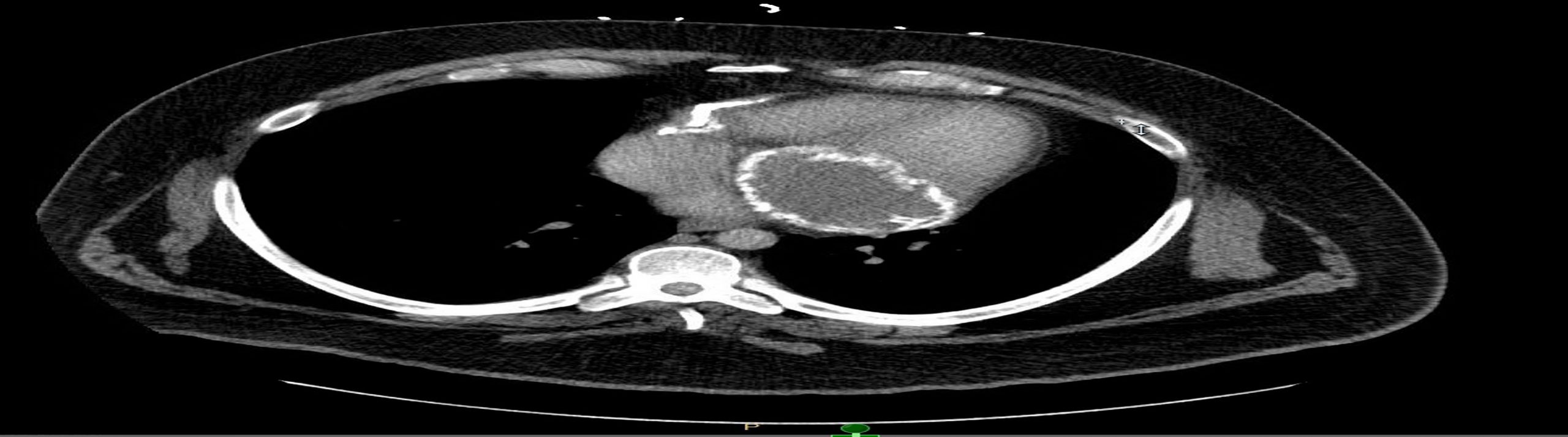
Case Presentation: Patient was a 37 year-old gentleman with history of recently diagnosed heart failure, hypertension, non-Hodgkin’s lymphoma s/p chemotherapy and prior methamphetamine use who presented with chest pain. He reported a history of heart failure but had never had cardiac imaging. This diagnosis had been made clinically based on lower extremity edema. He had been managed with lisinopril and furosemide. Patient reported anginal chest pain and stable lower extremity edema upon admission. His initial ECG revealed inferolateral T-wave inversions. Serial cardiac enzymes were negative. A transthoracic echocardiogram revealed a large extracardiac mass compressing the left atrium and left ventricle posteriorly. Left ventricular ejection fraction was normal at 55%. Stress myocardial perfusion imaging revealed no evidence of ischemia, but fixed defects within the anterior and inferior walls. Patient subsequently underwent CT chest, cardiac MRI, and transesophageal echocardiogram which all revealed a 7×9 cm homogenous inferior pericardial mass extending behind the left atrium (in the atrioventricular groove) and inferior aspect of the left ventricle. Patient underwent a partial pericardiectomy revealing an underlying pericardial cyst. 250 mL of fluid was drained. Infectious studies from the cyst material were negative. Pathology showed heavily calcified fibromembranous tissue. Patient suffered post-operative cardiogenic shock for which he briefly required inotropic support and aggressive diuresis. He did well thereafter and 6 months post-operatively his heart failure symptoms had completely resolved.
Discussion: Pericardial cysts occur with an incidence of 1 in 100,000 patients. Seventy percent arise in the right cardiophrenic angle. Symptoms can include shortness of breath, right heart failure secondary to compression, infection, and bleeding. Asymptomatic pericardial cysts can be observed, but resection may be needed if the diagnosis is not completely established by imaging. Simple drainage is generally not recommended, because these cysts typically recur without complete resection.
Conclusions: This patient suffered from a constrictive pericarditis, clinically resulting in heart failure. A pericardial cyst and its calcified membrane resulted in compression of his heart chambers and rigidity of the pericardium as a whole. This resulted in failure of the heart to relax normally in diastole, causing congestive heart failure. Once this constriction was relieved with resection of the cyst, the patient’s heart failure symptoms resolved. This case speaks to the importance of determining the etiology of a patient’s heart failure. This patient had an inadequate initial workup, and was simply placed on medical therapy. Further investigation revealed a reversible cause, and patient was able to return to his prior state of health after intervention. While a less frequent cause of heart failure, pericardial disorders and specifically pericardial cysts should be recognized as a potential etiology.