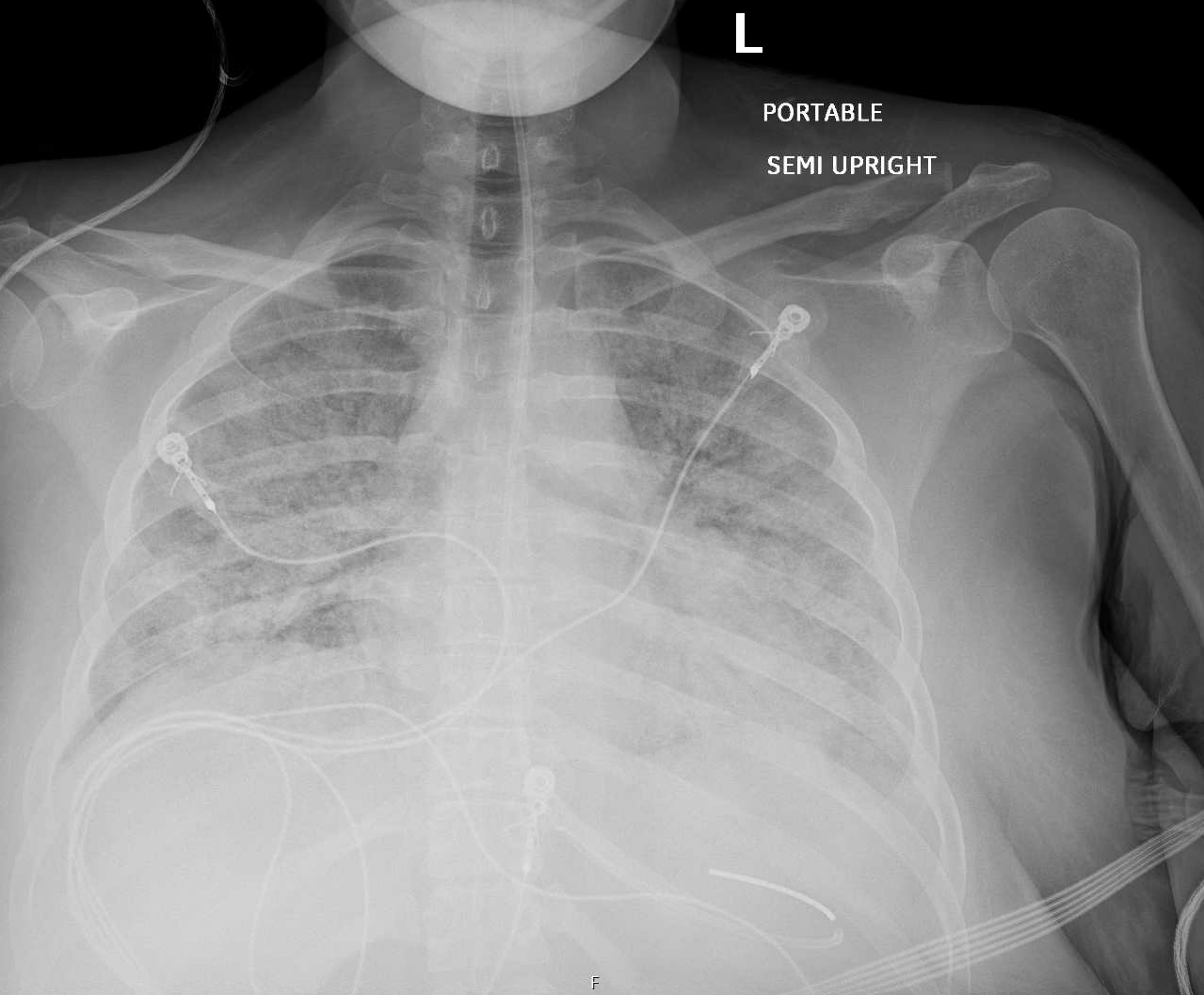
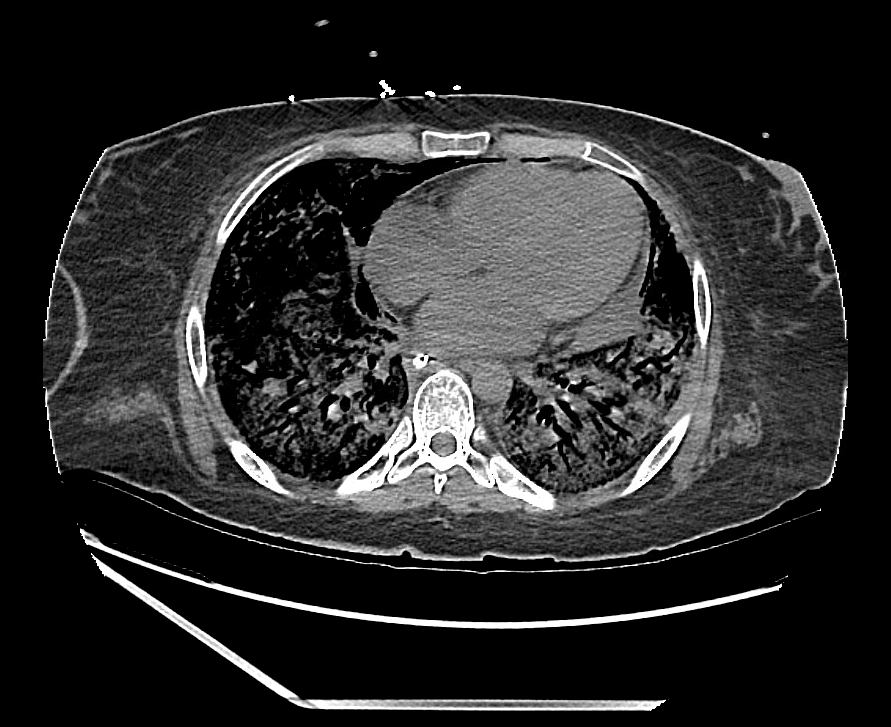
Case Presentation: 25-year-old female with PMH of anxiety, depression and daily vape use of 1 g of THC was admitted to the hospital for acute hypoxic respiratory failure requiring intubation. Chest x-ray and CT imaging confirmed diffuse bilateral opacities. Infectious workup including influenza, RSV PCR, bronchioloalveolar lavage (BAL) and blood cultures were negative. Rheumatological work up was benign. Cardiac enzymes were normal and TTE showed mildly reduced ejection fraction. A diagnosis of EVALI was made based on classical history, imaging findings and negative infectious workup. She was treated with empiric antibiotics and steroids however given rapidly increasing ventilatory support for ARDS she was transferred to a higher level of care facility for initiation of ECMO and lung transplantation candidacy evaluation. Unfortunately the patient was not a suitable candidate for transplant and despite aggressive measures including ECMO continued to have progressive clinical decline and was eventually transitioned to comfort care.
Discussion: Vaping is the inhalation of an aerosol produced by heating a solution containing nicotine or cannabis with devices such as e-cigarettes. The use of e-cigarette or vaping products is associated with an outbreak of severe lung injury in the United States especially affecting less than 35 year old males who used THC containing products. The CDC refers to this condition as e-cigarette or vaping product use associated lung injury (EVALI) which was first diagnosed in 2019. Pathogenesis is unclear but proposed mechanisms include airway centered chemical pneumonitis caused by inhalation and exogenous lipoid pneumonia due to deposition of aerosolized oils resulting in inflammatory response. EVALI is a diagnosis of exclusion and case definitions for confirmed and probable EVALI proposed by CDC are for surveillance purposes and not for clinical diagnosis.The current proposed criteria for EVALI include use of e-cigarettes along with pulmonary infiltrates on imaging in the absence of pulmonary infection and without evidence for a plausible alternative diagnosis (cardiac, rheumatologic and/or neoplastic). Clinical manifestations include respiratory, GI and constitutional symptoms including fever, weight loss, cough, dyspnea, abdominal pain, nausea, vomiting and diarrhea. Differential diagnoses including eosinophilic or lipoid pneumonia, hypersensitivity pneumonitis, and alveolar hemorrhage should be ruled out in the appropriate clinical context. Management involves supportive care with oxygen support, systemic corticosteroids, ventilation, and rarely ECMO.
Conclusions: EVALI has become a public health concern due to increasing prevalence in youth and patients should be counseled on the risks of vaping, including EVALI. Federal agencies like CDC and FDA recommend that healthcare providers should report suspected cases of EVALI to their state and local health department. Additionally, the CDC advises against the use of THC-containing vapes. Given limited data on EVALI and ECMO treatment there is a need for further studies for formulation of management guidelines to prevent severe consequences as our patient despite using additional therapies including ECMO had a fatal outcome. Patients with EVALI require an interprofessional healthcare team to address their needs holistically, optimize their care, and improve outcomes.