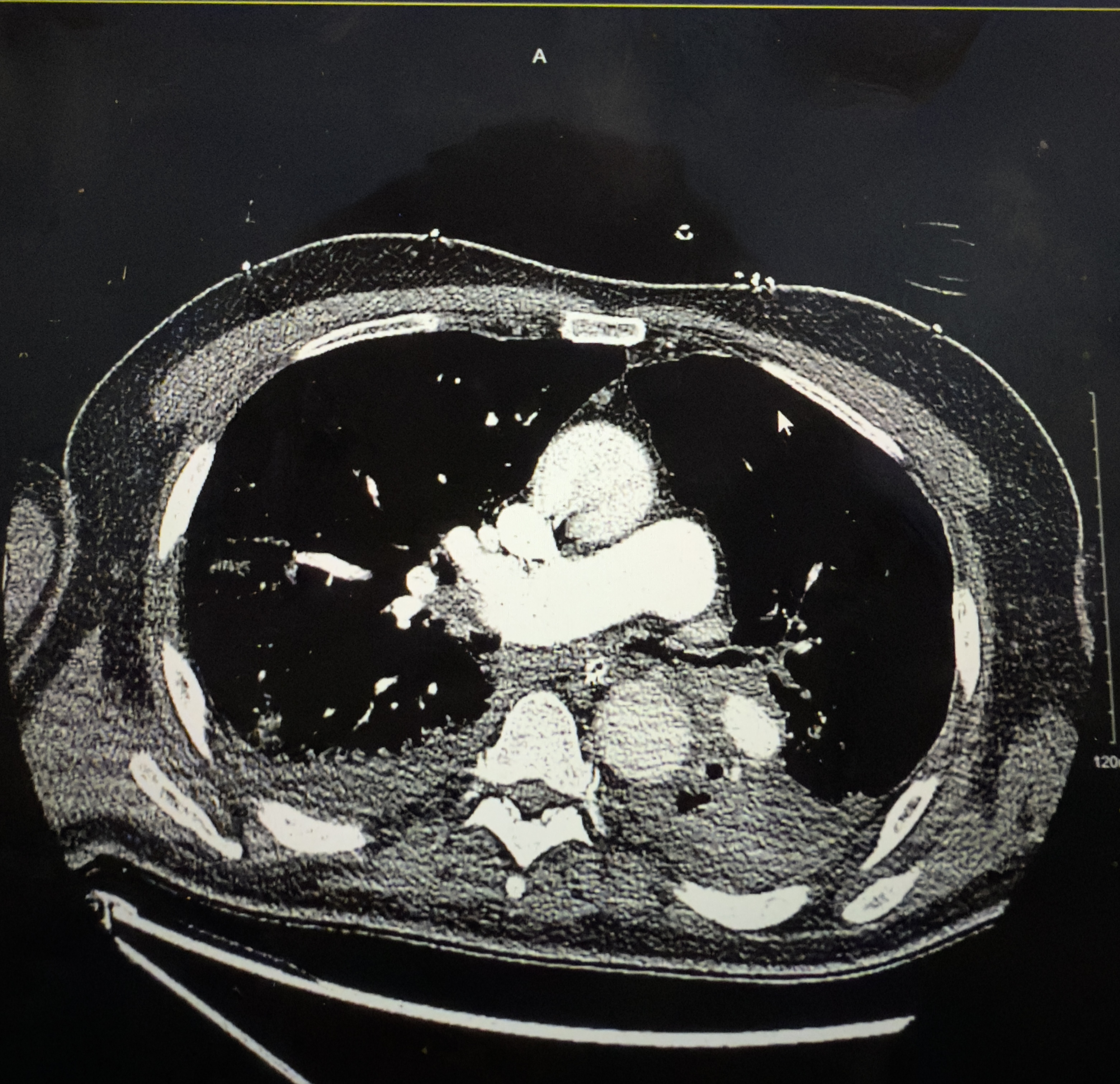
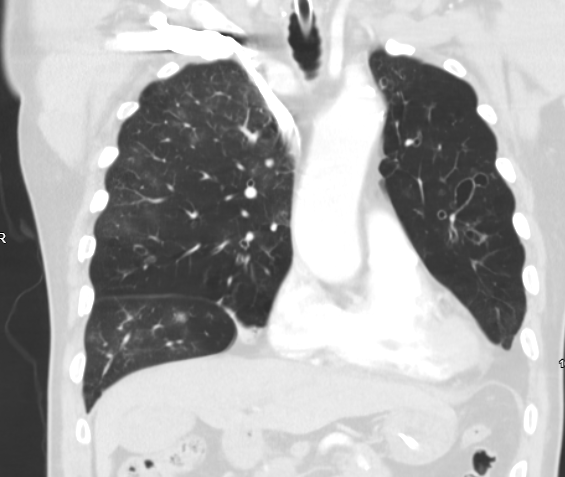
Case Presentation: A 70-year-old male with a history of chronic bronchiectasis and prior smoke inhalation lung injury presented with presumed hematemesis, but was quickly found to have large-volume hemoptysis. He became unstable and required emergent intubation. Initial Bronchoscopy showed blood clots bilaterally, but no active source; repeat bronchoscopy localized bleeding to the left lower lobe. Patient was given nebulized TXA and local epinephrine, and IR was consulted for Bronchial Artery Embolization (BAE), which achieved temporary hemostasis. Angiography identified hypertrophied and tortuous bronchial arteries with aneurysmal dilatation bilaterally. After extubation, He had recurrent massive hemoptysis necessitating re-intubation and repeat BAE. Shortly afterwards, he developed worsening hypoxia and a submassive pulmonary embolism (PE). With no further bleeding noted, anticoagulation was cautiously started, but led to another episode of massive hemoptysis within 24 hours. Anticoagulation was stopped, and an IVC filter was placed. Due to Bilateral Disease and recurrent bleeding, he was not a surgical candidate for lobectomy and remained ventilator dependent.
Discussion: Commencement of anticoagulation in a patient with active or recently controlled bleeding presents a significant challenge in hospital medicine. While pulmonary embolism requires timely intervention to prevent morbidity and mortality, massive hemoptysis itself is a life-threatening condition where anticoagulation aggravates it and can result in fatal consequences. This case highlights the difficult balance between controlling bleeding and treating thrombosis.In the setting of massive hemoptysis, the primary clinical goal is to achieve and maintain hemoptysis. Only after controlling the bleed, physicians reassess the safety of starting anticoagulation. Even after minimal invasive procedures such as bronchial artery embolization, the risk of rebleeding remains significant, particularly in patients with chronic structural lung disease. Therefore, the timing of anticoagulation initiation remains debatable and demands a multidisciplinary approach and individualized risk-benefit assessment. Current guidelines provide limited evidence for patients who simultaneously require anticoagulation and present a high bleeding risk. The Clinical approach must include:Stabilization of bleeding with interventions Severity of thrombotic burden (g., massive or submassive Pulmonary embolism)Risk of recurrent thromboembolism without anticoagulation or worsening of clot burden Possible alternatives to anticoagulation, such as temporary IVC filter placement Multidisciplinary input including pulmonary, surgical, Interventional radiology, critical care, and hospital medicine
Conclusions: This case highlights the challenge of initiating anticoagulation in a pulmonary embolism patient in the setting of active or high-risk bleeding. The decision to initiate anticoagulation in such patients requires a careful reassessment of bleeding control, multidisciplinary inputs, and individualized risk-benefit evaluation. This case demonstrates that further study and research is needed to guide the timing of starting anticoagulation and management protocols, including the role of alternative interventions such as IVC filter or any other alternatives for patients facing concurrent life-threatening hemorrhages and thromboembolic disease.