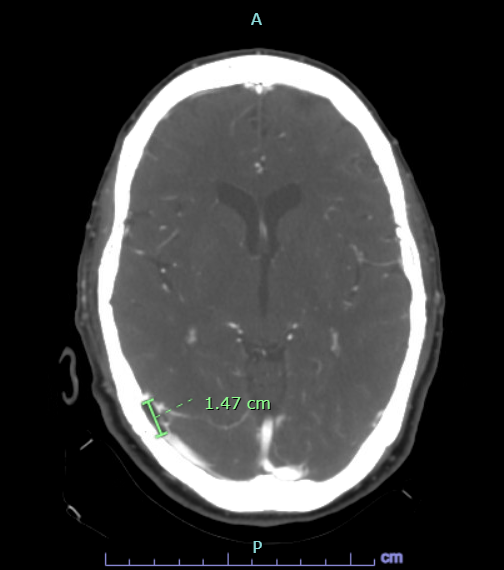
Case Presentation: A 70-year-old female with a past medical history of hypertension, irritable bowel syndrome, hyperlipidemia, and migraines on Carbamazepine since age 30 who presented to the emergency department (ED) with recurrent headaches for the past week. Initially responded to Advil but it became worse which prompted her to come to ED. Denied any photophobia or phonophobia. But mentioned she has pulsatile pain behind her right eye associated with nausea. She does have an extensive hypertensive history for which she got worked up for on previous admissions. She does not have any sensory or motor deficits. No history of falls. She is non-smoker, occasional alcohol use, and no illicit drug use. CT head and CXR were negative. Multiple rapids were called for severe headaches which resolved symptomatically with medical therapy. Triptans were avoided for medical management as patient was found to be hypertensive. MRI brain showed possible arteriovenous malformation (AVM) in the right cerebellum. CT venogram with suspected arachnoid granulation extrinsically compressing the right transverse/sigmoid sinus mimicking sinus venous thrombosis. MR Venogram negative. Patient underwent high volume LP and was found to have elevated opening pressure of 31 cm H2O. This alleviated the headache. She was discharged on Diamox with outpatient follow up with Neurology.
Discussion: Arachnoid granulations (AG) are composed of dense collagenous connective tissue that includes clusters of arachnoid cells in a delicate network within the vascular space filled with cerebrospinal fluid (CSF) from the contiguous subarachnoid space. This cell layer is continuous with the underlying arachnoid membrane. Growth of arachnoid membrane-like projections into the dural sinus are called arachnoid villi or AG, depending on size. CSF is synthesized and produced by the choroid plexus, where it circulates to the subarachnoid space and eventually returns to the venous blood via AG. AG are most commonly seen at the junction between the middle and lateral thirds of the transverse sinuses, (92%) near the entry sites of the superficial veins. Differential diagnosis of a mass within the dural sinus include meningioma, inclusion tumor, sinus cavernoma, and meningocele, which can be excluded by characteristic imaging findings. It is particularly important to differentiate AG from dural sinus thrombosis, which may cause a fatal outcome and requires an immediate approach. Thrombosis usually involves an entire segment of a sinus or multiple sinuses, and can extend to the cortical veins, whereas AG produce focal, well-defined, nodular defects in the sinuses. Typical MRI finding of dural sinus thrombosis is a clot in the sinus that is iso- to hyperintense on T1-weighted imaging and hyperintense on T2-weighted imaging. A key MRI feature of giant AG is a nonenhancing lesion with central linear enhancement and surrounding blood flow on contrast enhanced MR venography. Thrombus within the sinus may show contrast enhancement and venous flow occlusion.
Conclusions: In conclusion, it should be kept in mind that giant AG may be misdiagnosed as dural sinus thrombosis, which requires immediate approach with anticoagulation and thombolysis/thrombectomy for severe cases. Before diagnosing focal, nodular defect in the sinuses as thrombosis, giant AG should be considered as a differential diagnosis. MRI and contrast-enhanced MRI venography are the most useful diagnostic tools to differentiate giant AG from dural sinus thrombosis.