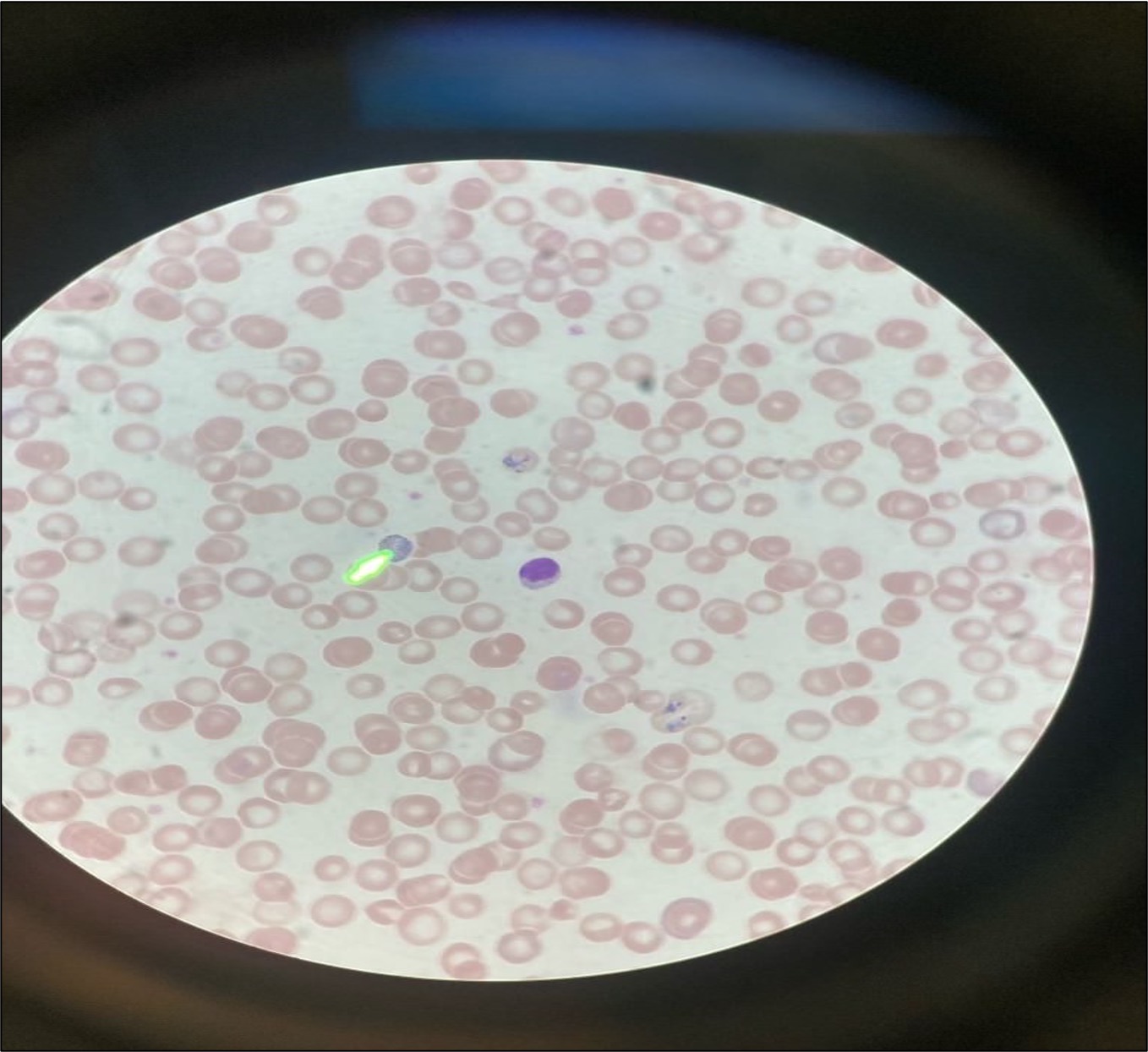
Case Presentation: A 58-year-old man originally from Ethiopia with severe disability from a recent stroke presented to the Grady Emergency Department from a nursing facility with fever, tachycardia, and hypotension. Additional medical history includes hypertension, type 2 diabetes, latent TB infection undergoing treatment, and malaria infection within the last year. His initial workup showed lactic acidosis, normocytic anemia, and increased reticulocytes. He was treated for septic shock of unknown origin with vancomycin and piperacillin-tazobactam, but he continued to have cyclic fevers despite antibiotic therapy. An incidental finding on blood smear showed parasitemia, which led to a diagnosis of relapsed malaria infection with Plasmodium vivax species. After consultation with clinical pharmacists, he was treated with high-dose atovaquone-proguanil and primaquine. He had clearance of parasitemia after four days of therapy and was discharged. He was asymptomatic at multiple follow-up appointments and had a negative malaria smear one month after discharge.
Discussion: Several factors complicated the selection of anti-malarial therapy for this patient. First-line agent artemether-lumefantrine was not viable due to drug-drug interactions with rifampin. Second-line agent chloroquine was not viable due to resistance in Ethiopia. Given the pharmacokinetic constraints, high-dose atovaquone-proguanil was chosen to treat his acute infection. Despite increased metabolism of atovaquone-proguanil due to rifampin, he had clearance of parasitemia after 4 days of therapy. For treating residual hypnozoites, first-line agent tafenoquine could not be used due to procurement issues, leading to the choice of a 14-day course of primaquine. Ultimately, he was seen at 1- and 3-month follow-ups with no evidence of repeat relapse.
Conclusions: For patients with history of malaria infection with P. vivax or P. ovale, it is advantageous to include relapsed infection in differential diagnosis of any new febrile illness. Additionally, drug-drug interactions, potential resistance in the region of transmission, and medication availability are all important considerations for selecting an effective anti-malarial therapeutic regimen.