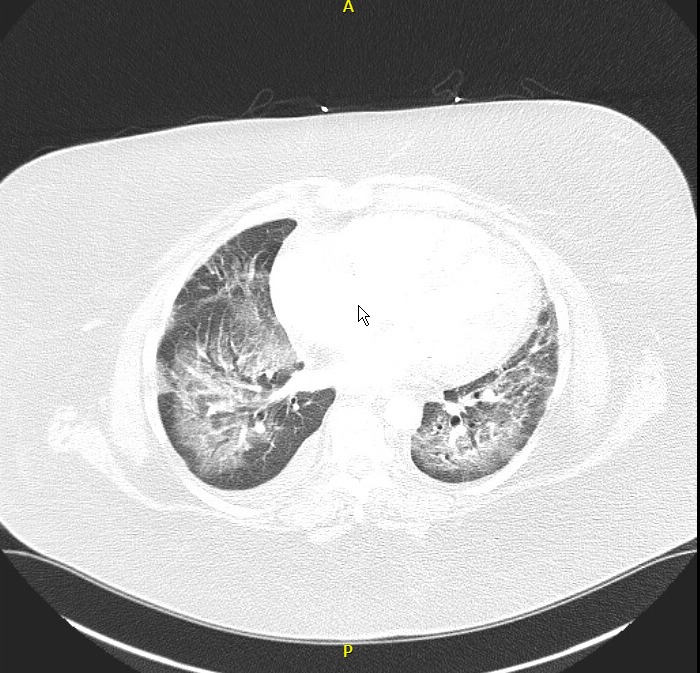
Case Presentation: A 59-year-old Caucasian woman with asthma and PsA, treated with monthly guselkumab injections, presented with a one-week history of progressive shortness of breath and generalized weakness. Initial laboratory findings revealed leukocytosis and lactic acidosis, and arterial blood gas (ABG) indicated respiratory acidosis. Chest X-ray showed bilateral ground-glass opacities, and echocardiography revealed preserved ejection fraction without diastolic dysfunction. A chest CT scan showed ground-glass opacities concerning for DAH.Despite initial BiPAP support and empiric antibiotics, her condition deteriorated, necessitating mechanical ventilation. Bronchoscopy with bronchoalveolar lavage (BAL) revealed progressively bloody fluid, confirming DAH. Infection and autoimmune workups, including a vasculitis panel, were negative, implicating guselkumab as the likely cause.Surgical lung biopsy was not performed due to the patient’s tenuous respiratory status. The patient was treated with pulse-dose corticosteroids, followed by a tapering regimen. Due to severe hypoxemia, she required extracorporeal membrane oxygenation (ECMO) support for one week. She was successfully weaned off oxygen.Unfortunately, during recovery, the patient developed ischemic bowel, leading to a complicated clinical course. After further deterioration, the family decided to transition to comfort care, and the patient passed away.
Discussion: This case highlights the rare but severe complication of DAH associated with guselkumab. Although biologics targeting IL-23 have proven effective in treating moderate-to-severe psoriasis and PsA, rare respiratory complications like DAH must be considered when patients present with acute respiratory distress. Negative infection and autoimmune workups in this case pointed to guselkumab as the causative agent.The patient’s condition improved with corticosteroid treatment, ECMO support, and gradual weaning from oxygen. However, her recovery was complicated by ischemic bowel, a factor that contributed to her eventual death. This case reinforces the importance of early diagnosis and management of severe complications during biologic therapy, particularly in patients with complex medical histories.
Conclusions: Guselkumab is a highly effective treatment for PsA and psoriasis, but clinicians should remain vigilant for rare, life-threatening complications like DAH. Early recognition and treatment, including corticosteroids and mechanical support, may improve outcomes, but the risk of severe complications underscores the need for close monitoring of patients undergoing biologic therapy.