
Background: Residents, because they are on the frontlines of the provision of care, are integral to improving care. Yet the Accreditation Council for Graduate Medical Education (ACGME) has reported residents are not as engaged in improving patient safety as they could be, noting, “Though most residents and fellows were aware of their [clinical learning environment]’s process for reporting patient safety events, fewer of them appeared to have used it themselves to report events.” We have made this observation at our academic medical center, where residents in the Department of Internal Medicine report an average of 7 safety events per month (N = 87 over 12 months).
Purpose: The goal of this innovation was to increase the number of patient safety reports filed by internal medicine residents from an average of 7 per month to an average of 21 per month over the first 2 months and sustain this average over 10 additional months.
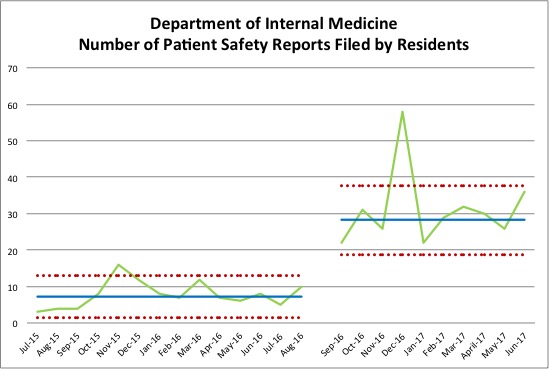
Description: As part of a two-week quality improvement (QI) curriculum, senior residents conduct proactive patient safety rounds weekly by visiting team rooms and asking if there have been any safety issues. If a resident verbally reports an event during the safety rounds, the senior resident can help them file using the institution’s online reporting system. In addition, the senior resident is able provide peer coaching regarding what types of safety events should be filed and when to escalate serious safety events to program leadership. A total of 298 patient safety reports were filed by internal medicine residents during the intervention. Patient safety reports by residents increased from a mean of 7.86 (± 3.63) reports per month to a mean of 31.20 (± 10.39) reports per month, p< 0.0001. The statistical process control chart demonstrated 10 months of sustained change.
Conclusions: Residents are key individuals for reporting safety events, yet reporting is low nationally. Resident-led safety rounds tripled the rate of safety event reporting. This relatively simple innovation overcomes several barriers to patient safety reporting by residents. First, it prompts residents to recall safety issues. In addition, residents receive peer coaching, which reduces the initial unfamiliarity with the reporting system and makes the task less overwhelming. Finally, the QI resident is available to educate on the types of safety issues that are important to report but may be under-recognized by residents who are still developing basic patient safety awareness.
.jpg)