Background: Day-to-night inpatient handoff is a high-risk moment, with potential for miscommunication. A novel handoff program recently reduced medical errors and preventable adverse events. Historically, handoffs performed by Internal Medicine residents at our institution were not standardized and there was little workplace-based performance feedback. We evaluated the impact of a novel standardized handoff tool and direct handoff observation and performance feedback on handoff quality. We also investigated the impact of other factors such as number of patients, handoff pace, and handoff location on the quality of handoff encounters.
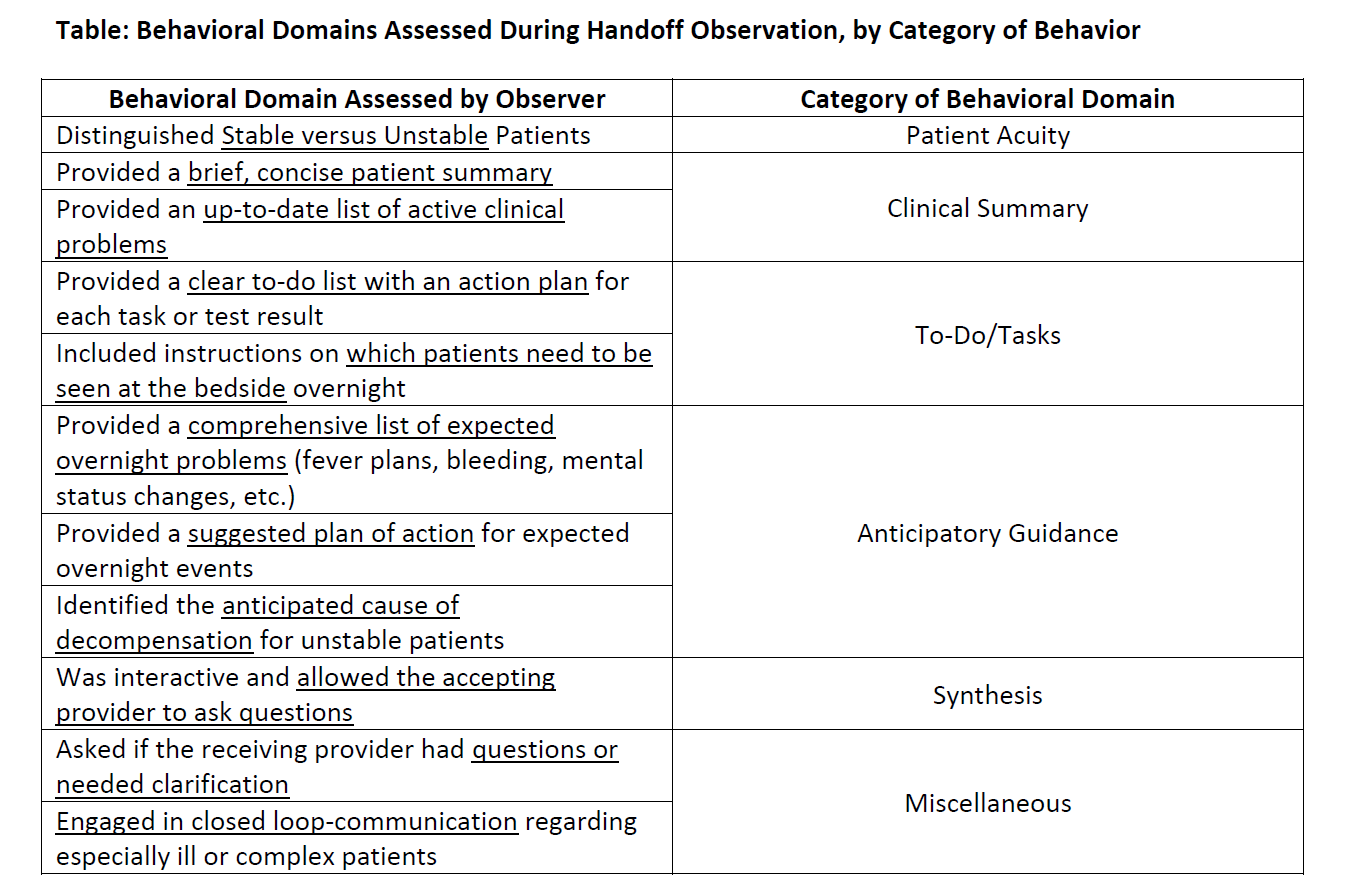
Methods: Inpatient ward teams were observed performing day-to-night handoffs during the baseline (January-April 2015) and intervention (April-June 2015) periods. The intervention consisted of a tool that prompted providers to write a patient summary, to-do list, and critical take-home messages, and provided organ system-specific anticipatory guidance for potential overnight events. Feedback was provided on an ad-hoc basis during the baseline period and uniformly during the intervention period. Team performance was evaluated by the same observer for adherence to 11 behaviorally-anchored domains based on best practices (Table 1), and each behavior was rated on a 4-point scale (seen for all, most, some, or no patients on the team) using a rubric adapted from the literature. The primary outcome was each team’s composite score, expressed as a percentage of 44 possible points. The impact of the intervention and categorical factors (service type, handoff location, handoff pace) were assessed using ANOVA/T-tests. Continuous predictors (number of patients/team, number of providers/team, patient-to-provider ratio) were assessed generalized linear models. Multivariate generalized linear models were used to assess significant univariate predictors.
Results: 99 teams were observed during the baseline period, and 52 teams were observed during the intervention. Feedback was provided to 55% of teams at baseline, and 100% of teams during the intervention. The intervention increased the composite score from 72.5% at baseline to 92.3% during the intervention (p<0.0001). The number of patients per team was inversely related to performance, with each additional patient associated with a 1.73% decrease in score (p=0.0002). Service type predicted performance (p=0.05); general medical teams performed worse than subspecialty or mixed general medical/subspecialty teams. Ideal handoff pace was associated with higher scores than slow or fast pace (p<0.0001), and handoffs performed in a dedicated room were associated with higher scores than those performed in the hallway (p<0.0001). In the multivariate model, the handoff intervention remained the strongest predictor of performance.
Conclusions: An intervention consisting of a structured handoff tool and direct observation and feedback of resident handoffs improved handoff quality. Improvement was independent of team census, handoff location, and handoff pace. These results suggest that the tool in combination with direct observation may improve the adherence to best practices, and support the use of direct observation in medical education.