Case Presentation: A 20 year old woman with a history of astrocytoma of thoracic and lumbar spine status post resection with subsequent neurogenic bladder and bowel presented with acute encephalopathy following a viral illness. Initial workup showed acute kidney injury (creatinine 2.21 mg/dL), normal hemoglobin (12 g/dL), new thrombocytopenia (platelet 60 K/uL), and urinalysis suggestive of UTI. CT scan of brain, spine, abdomen, and pelvis showed no acute abnormality. On exam, she was lethargic and confused with low respiratory rate of 5-6 with apnea. Urine culture was positive for E. coli, for which patient was treated with antibiotics. On hospital day 3, hemoglobin and platelet decreased to 5.4 g/dL and 16 K/uL. Peripheral smear showed schistocytes with low haptoglobin and elevated LDH consistent with hemolytic anemia. Her clinical presentation was concerning for atypical Hemolytic Uremic Syndrome (HUS) vs. Thrombotic Thrombocytopenic Purpura (TTP). Hematology recommended plasma exchange (PLEX) and high dose 60 mg daily of IV Solumedrol. With PLEX treatment, mental status returned to baseline while anemia and thrombocytopenia gradually improved. Stool test was positive for shiga-toxin and ADAMTS-13 level returned >100%. This finding was more consistent with typical ST-HUS, thus PLEX and steroids were discontinued after 2 days. Patient continued to make slow improvement and was eventually discharged to inpatient rehab facility.
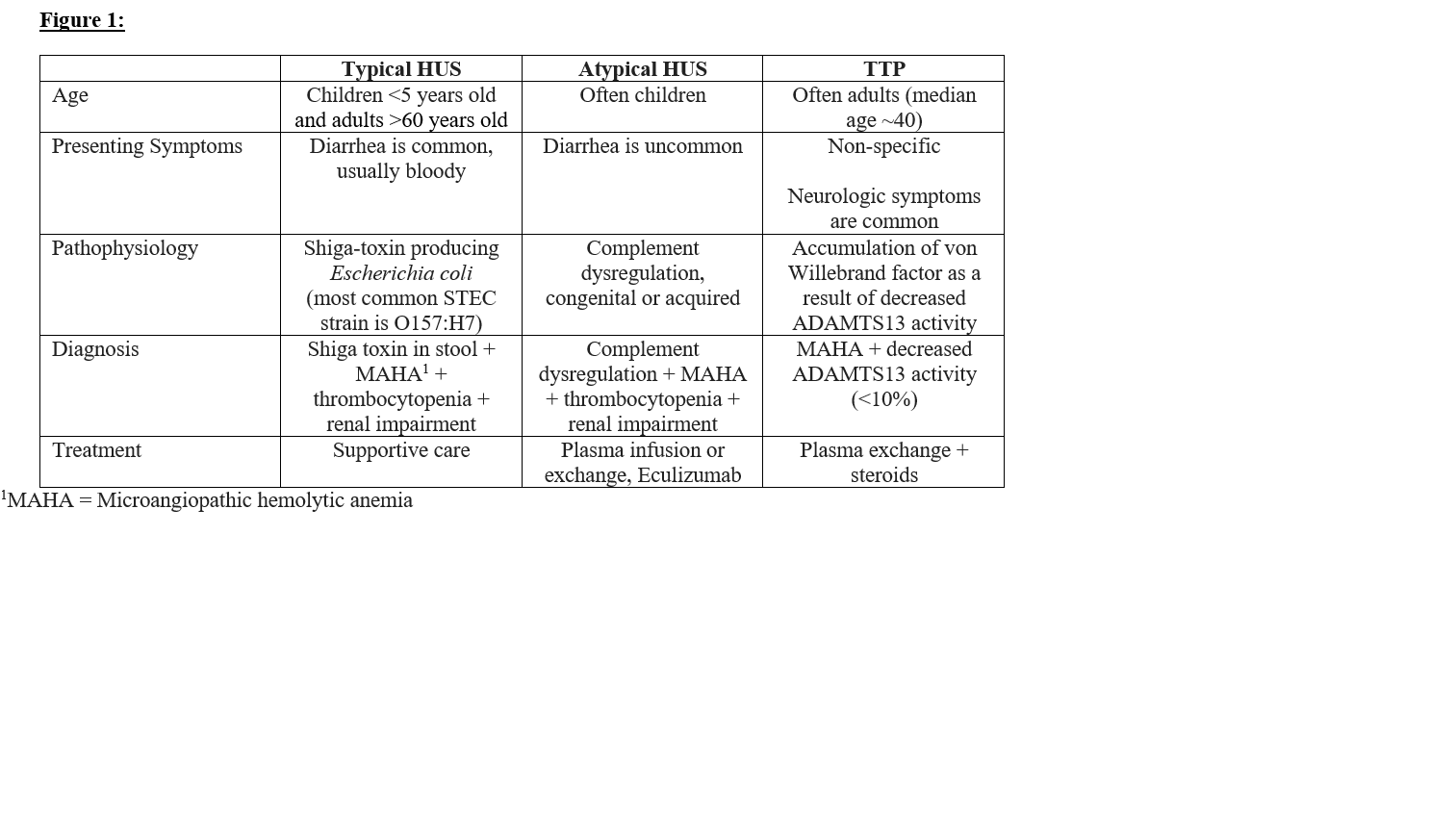
Discussion: Shiga toxin-producing E. coli infections are common across all age groups. However, HUS occurs most frequently in children <5 years old and adults >60 years old. Children with ST-HUS typically present with a prodromal illness with abdominal pain, vomiting, and bloody diarrhea 5-10 days prior to development of HUS. Adults often present similarly, however they more commonly have non-bloody diarrhea or no diarrhea at all.HUS is characterized by a triad of hemolytic anemia, thrombocytopenia, and acute kidney injury. Diagnosis of ST-HUS can be confirmed with stool culture selective for STEC and a Shiga toxin immunoassay. It is important to note that other TMA syndromes such as TTP and atypical HUS can present similarly to ST-HUS. Renal involvement is less common in TTP, and this diagnosis can be ruled out with normal ADAMTS-13. Greater than 15% ADAMTS13 levels make TTP unlikely, while positive Shiga-toxin immunoassay can confirm ST-HUS. Atypical HUS is characterized by dysregulation of complements.
Conclusions: It is important to differentiate between ST-HUS, atypical HUS and TTP as clinical management is different. ST-HUS is typically managed with supportive care, while atypical HUS and TTP are managed with plasma exchange therapy and consideration for Eculizumab for atypical HUS.