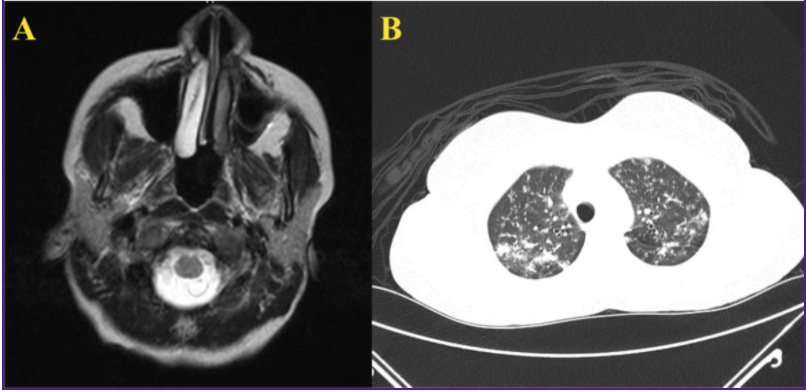
Case Presentation: A 36-year-old Kenyan female, who immigrated to the United States 18 months ago, with no significant past medical history presented to our hospital with worsening occipital headaches. 6 months prior, she had a CT scan and MRI of the brain that revealed a stable right-sided cerebellar mass. Now, she endorsed a recent history of unintentional weight loss. At this time, the patient had no history of cough, known history of tuberculosis positive contacts or any other respiratory symptoms. The patient was vitally stable and neurologically intact with an unremarkable respiratory exam and no lymphadenopathy. Labs at this time were unremarkable and a CSF analysis performed was normal. To investigate a possible metastatic tumor, the patient had a CT chest which showed bilateral diffuse reticulonodular opacities in a “tree-in-bud pattern” (Figure -1B) with bi-apical patchy opacities. A repeat MRI brain performed showed showed a conglomeration of three 7mm ring-enhancing nodular lesions in the cerebellum (Figure-1A). These were deemed too small to biopsy. A bronchoscopy was performed that showed no visually appreciable gross abnormalities. Bronchial washings showed 3+ acid-fast bacilli and a subsequently positive TSPOT. The patient was diagnosed with miliary tuberculosis and was started on RIPE therapy.
Discussion: Brain tuberculomas are very rare with MRI being the study of choice. CT scans of the lungs in TB patients indicating the “tree-in-bud” pattern has been shown to be a primary sign of abnormality. Miliary tuberculosis is the widespread dissemination of Mycobacterium tuberculosis via hematogenic spread that usually follows primary infection, with no or only a short latency. Interestingly, our patient had a latency period of at least 18 months. This is important from both a public-health standpoint as well as for the patient since untreated miliary TB has an assumed mortality of 100% while early treatment would reduce mortality to less than 10%. It is therefore important to have a very high index of suspicion with characteristic brain lesion such as ring-enhancing lesions on MRI which may suggest tuberculosis as an etiology, especially in those patients who have migrated from endemic regions.
Conclusions: Tuberculomas are brain abscesses secondary to tuberculosis (TB). There have been rare case reports of patients that presented with prolonged nonspecific symptoms and were found to have multiple brain tuberculomas. This case highlights the importance of obtaining travel history at the time of admission and encourages hospitalists to have a high index of suspicion in patients from endemic countries.