Background: Risk factors for hospital-acquired venous thromboembolism (HA-VTE) have been well-studied in adults, with validated risk assessment tools available. Adults admitted to children’s hospitals are younger but with comorbidities stemming from childhood conditions. There is a paucity of data on HA-VTE characteristics and risk factors in this population. Our objective was to evaluate HA-VTE in adult-aged (≥18 years) patients admitted to Cincinnati Children’s Hospital Medical Center.
Methods: We performed a single center case-control study encompassing a 4 year period (2013-2016). Cases of HA-VTE were defined as radiographic evidence of deep vein thrombosis (DVT) or pulmonary embolism (PE) that developed ≥48 hours after admission or within 30 days of hospital discharge. Controls were matched 2:1 on age and date of admission. Six reviewers abstracted data including patient characteristics, co-morbidities, VTE risk scores (Caprini and Padua), VTE characteristics, and outcomes. Wilcoxon-rank sum test was used for continuous variables and chi-squared or fisher exact tests were used for categorical variables. Conditional logistic regression was done to estimate the association of Caprini and Padua score with HA-VTE.
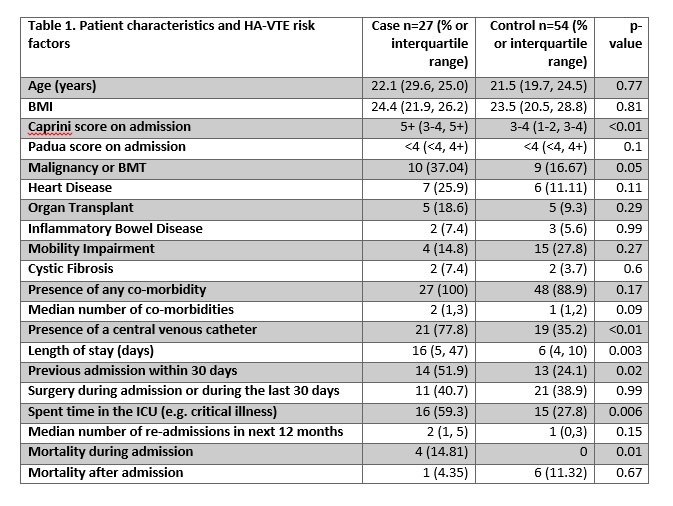
Results: Over the study period we identified 27 cases of HA-VTE, and 54 appropriate controls. 88.9% of events were DVTs and 11.1% were PEs. Patient characteristics and HA-VTE risk factors are presented in Table 1. Cases and controls had similar co-morbidities, except for malignancy, which was significantly higher in cases. The Caprini score on admission was significantly higher in cases than controls (p<0.01); the Padua scores were similar (p=0.1). As the Caprini score increased, odds of developing HA-VTE progressively increased (OR 0.96 95% CI 0.1-10.4 for 1-2 vs 0; OR 7.9 95% CI 0.8-78.9 for 5+ vs 0). Higher Padua score (≥4 vs <4) was also associated with increased odds of HA-VTE (OR 2.2 95% CI 0.8-5.8). These results did not reach statistical significance owing to small sample size. Pharmacologic and/or mechanical prophylaxis was given in 30% of cases and 28% of controls (p=0.86). In-hospital mortality was significantly higher in cases.
Conclusions: In this single center study, malignancy, critical illness, presence of central venous catheter, 30-day readmission, and longer length of stay were significant risk factors for HA-VTE in adults admitted to a children’s hospital. HA-VTE was associated with increased mortality. The Caprini score performed better than Padua at identifying patients at higher risk of clot, although with a small sample size there may be confounders which were not accounted for in the analysis. Future directions should include a multi-institutional study to determine if these results are more broadly applicable.