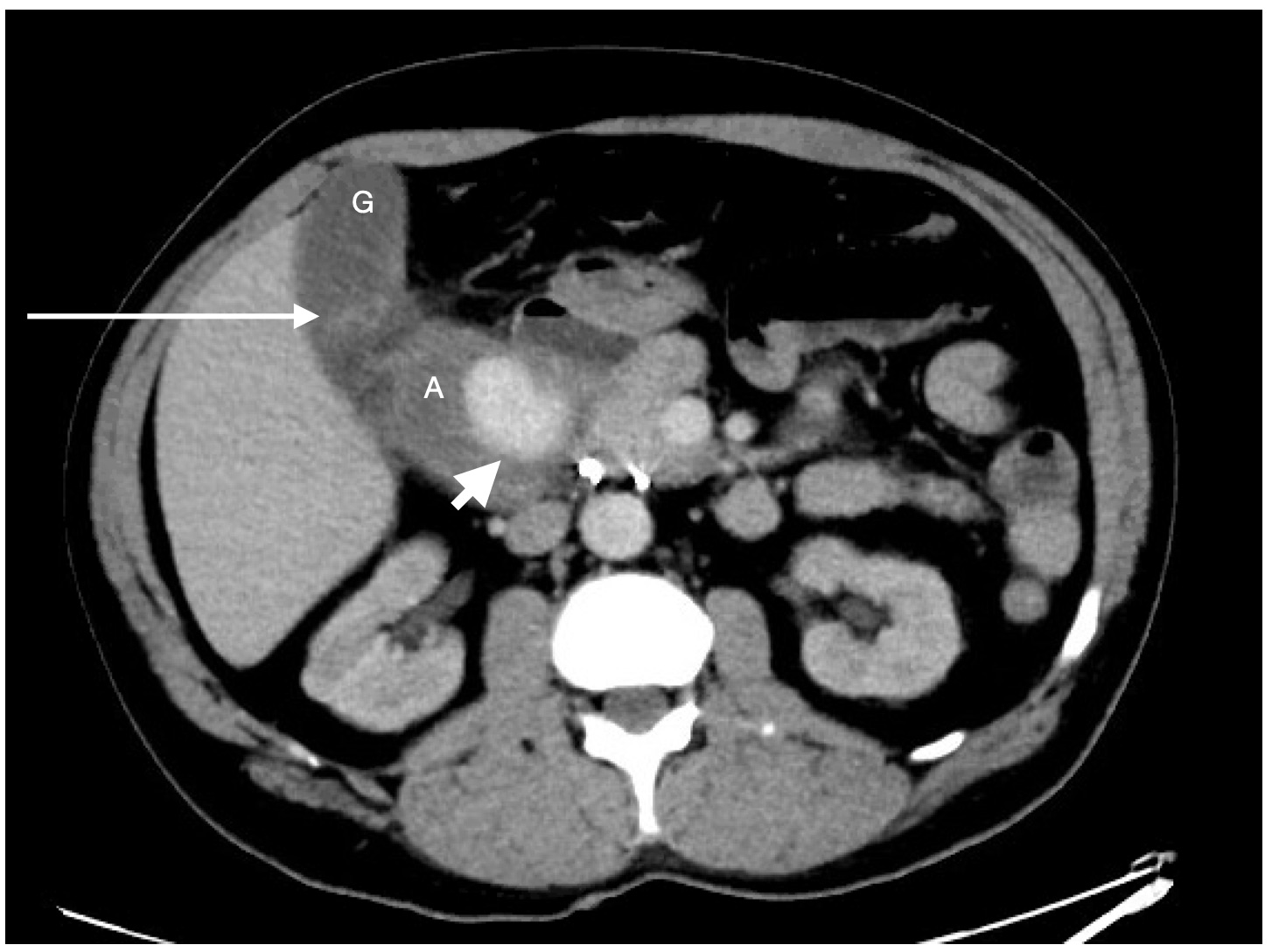
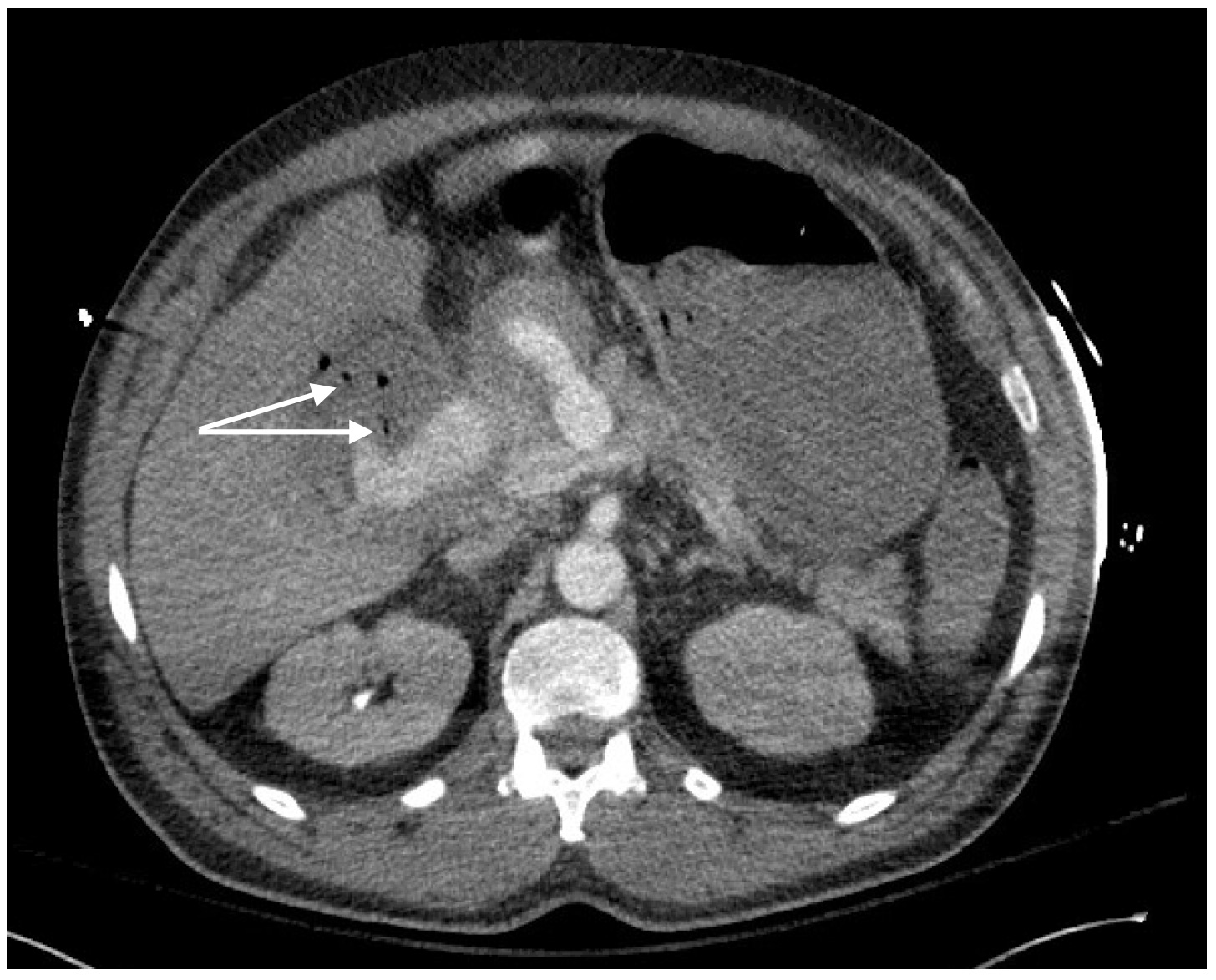
Case Presentation: A 51-year-old man with seropositive rheumatoid arthritis (RA) and chronic intra-abdominal arterial aneurysms attributed to RA-associated vasculitis presented with a one-day history of right upper quadrant abdominal pain and melena. His vital signs were within normal limits. Notable laboratory studies included hemoglobin 6.1 g/dL, total bilirubin 1.4 mg/dL, AST 161 U/L, ALT 217 U/L, and alkaline phosphatase 311 U/L. Computed tomography (CT) of the abdomen showed aneurysms of the left and right hepatic arteries and what appeared to be blood within the gallbladder (Figure 1). He developed massive hematemesis leading to pulseless electrical activity requiring cardiopulmonary resuscitation. After return of spontaneous circulation, a repeat CT showed no new aneurysm rupture or arterial dissection, but gas was now visible within a hepatic artery aneurysm abutting the gallbladder (Figure 2). These collective CT findings suggested a fistula between the gallbladder and aneurysm. He underwent embolization of the common, right, and left hepatic arteries followed by cholecystectomy and resection of the abutting aneurysm. Pathology of the aneurysm demonstrated segmental arterial mediolysis (SAM) without evidence of vasculitis. Prednisone previously started for presumed RA-associated vasculitis was discontinued. He did not develop any recurrent bleeding and was discharged home in good condition.
Discussion: The hospitalist should be familiar with SAM, a rare noninflammatory vasculopathy that causes degeneration of the medial layer of arteries and typically manifests as intra-abdominal artery dissections or aneurysms. There are no known risk factors. Presenting symptoms range from nonspecific abdominal pain to life-threatening intra-abdominal hemorrhage. Histopathology remains the lone means for definitive diagnosis. Though angiography may suggest SAM, vasculitis (especially polyarteritis nodosa) may present with an identical angiographic pattern. The possibility of RA-associated vasculitis in this patient made diagnosis impossible without histopathology. Treatment of SAM centers around surgical resection or embolization. There is no role for corticosteroids or immunosuppressants.
Conclusions: SAM is a rare cause of intra-abdominal arterial aneurysms and dissections. It should be suspected when other findings suggestive of vasculitis are absent. This distinction is critical as unnecessarily starting treatment for presumed vasculitis could result in significant harm. A situation in which a patient has a known condition associated with vasculitis may pose a significant diagnostic challenge that may be resolved only by biopsy of an aneurysm.