Background: Avoidable readmissions result in unnecessary hospital stays for patients, over utilization of beds, and increased waiting time for other patients. Multiple interventions have examined reducing readmissions, mostly focusing on pre-discharge and out of hospital post-discharge interventions. An additional potential target in reducing avoidable readmissions are the population of patients returning to the Emergency Department following a recent admission. At Northwell Health – Long Island Jewish Medical Center, the historical 30-day all-cause readmission rate for patients presenting to the Emergency Department following an index admission for Medicare fee for service patients over age 65 is 80%.
Purpose: To develop and implement a multidisciplinary pathway to decrease the 30-day readmission rate for Medicare patients age 65 and over returning to the Emergency Department in a large tertiary care academic teaching hospital. We hoped to decrease this rate as well as the overall readmission rate by preventing avoidable readmissions.
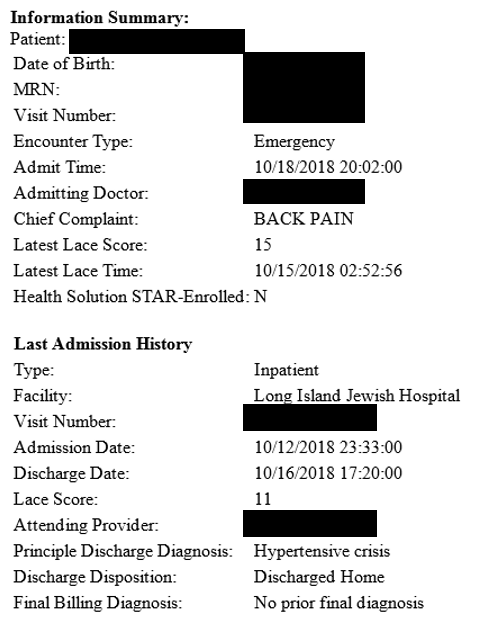
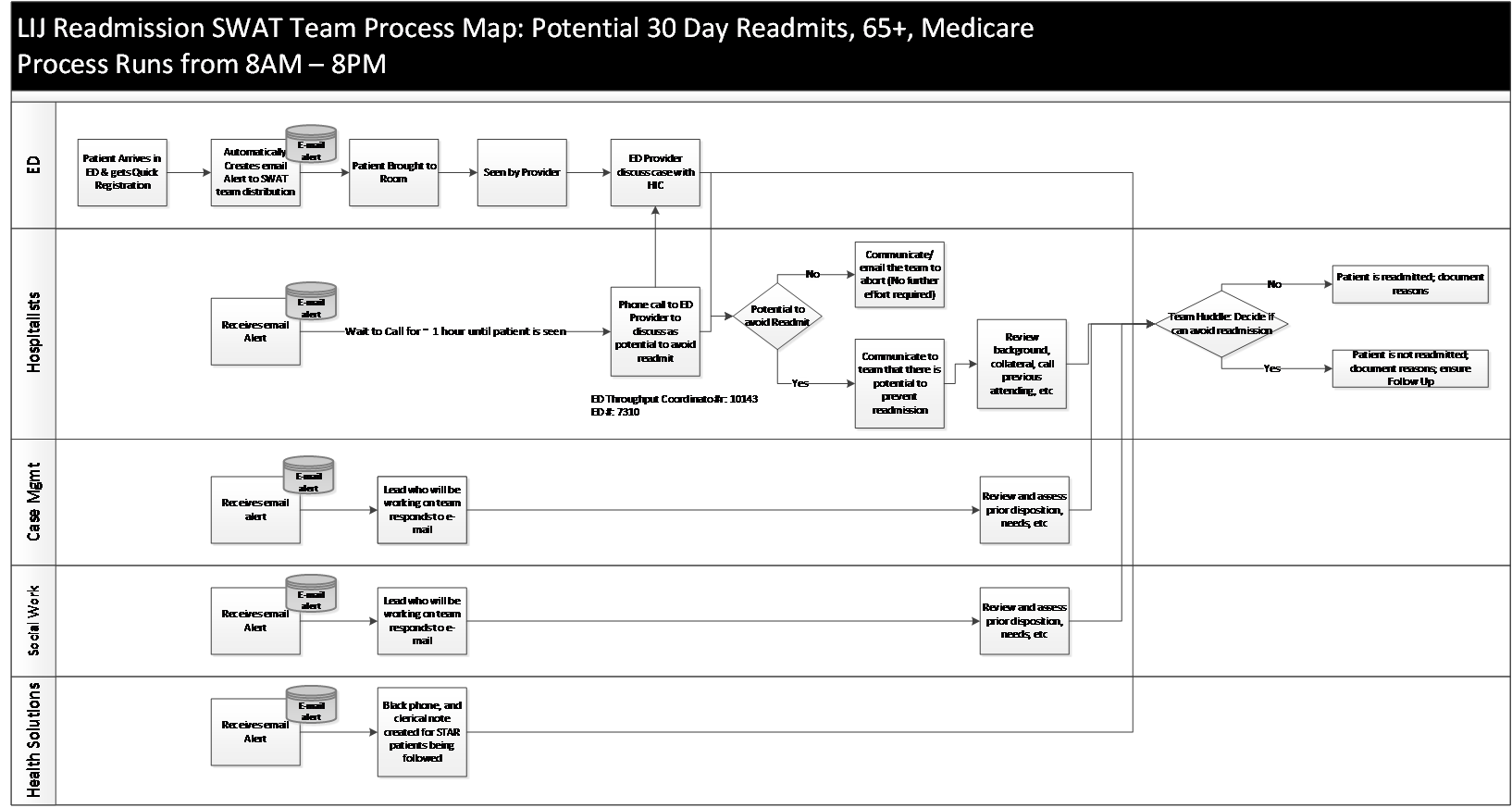
Description: A multidisciplinary “SWAT” Team was created consisting of hospitalists, emergency room providers, case managers and social workers. We utilized an alert system to notify the SWAT team providers via email (Figure 1) upon a patient’s registration in the emergency room and implemented a protocol (Figure 2) to facilitate the following: • Shared decision making regarding patient disposition
• Transitions of care
• Reduction in avoidable readmissions
Once the SWAT providers are notified of the patient’s arrival in the emergency room, the case managers and social workers assess the prior needs of the patient, emails this information to the SWAT group, and consults emergency room CM/SW if needed. In parallel, the hospitalist reviews information from the prior admission and contacts prior care providers. After the patient has been initially evaluated in the emergency room, the hospitalist has a verbal discussion with the emergency room provider. The providers discuss potential for avoiding readmission (sharing pertinent information from prior admission, need for bedside evaluation by prior attending physician, considering observation status, discharging the patient with close follow-up, etc). If the hospitalist and emergency room physician agree that readmission can be prevented, the entire SWAT team collaborates to create a safe disposition plan. The data is then recorded in a shared database.
The pathway was implemented in July 2018 and we have since noted a 13% reduction in 30-day All-Cause readmission rate for patients returning to the Emergency Department.
Conclusions: The creation of a multidisciplinary pathway to facilitate shared decision making for Medicare fee-for-service patients age 65 and over who present to the emergency room within 30 days of discharge can lead to reductions in their 30-day all-cause readmission rate. These reductions will likely improve patient care, quality, and reduce hospital costs. Further study is needed to determine if improvements in reduction of emergency room readmissions and 30-day all-cause readmissions are sustained and if this pathway can be expanded to all patients who present to the emergency room within 30 days of discharge.