Background: COVID-19 has placed an unprecedented strain on healthcare systems worldwide, increasing demand for critical care beds1. To address shortage of critical care beds, innovative methods to increase capacity are needed. At our large, urban academic safety-net hospital, patients with diabetic ketoacidosis (DKA) are admitted to critical care units for intravenous (IV) insulin administration and close monitoring. Alternatively, subcutaneous (SC) insulin protocols have been shown to be safe and effective in treating mild to moderate DKA2. Moreover, SC insulin protocols for DKA have been associated with reduction in hospital cost and resources likely driven by decreased ICU utilization2,3. We therefore piloted implementation of a SC insulin protocol to treat mild to moderate DKA on a general medicine ward.
Methods: We conducted a retrospective analysis of the data associated with the use of the SC DKA protocol to better inform quality improvement efforts directed at optimizing implementation of the protocol at our institution. The protocol algorithm, including inclusion and exclusion criteria were translated into order sets and embedded into our electronic health record. Patients with mild to moderate DKA were defined as those having an arterial PH between 7.0-7.3, HCO3 between 10-18 mmol/L, and B- Hydroxybutrate between 3-8 mmol/L. The initial SC bolus injection of insulin Aspart is 0.3 units/kg, followed by 0.2 units/kg (if CBG≥ 250 mg/dL) or 0.1 units/kg (if CBG < 250 mg/dL) every 2 hours. A dextrose 5% infusion is started for CBG < 250 mg/dL. IV fluids and electrolytes repletion were left to the discretion of the provider, as in our IV insulin protocol. CBG was monitored every 2 hours and a basic metabolic panel was checked every 4-6 hours until DKA resolution. A select group of nurses and hospital medicine physicians were trained on the protocol prior to rollout.We reviewed the charts of 20 patients admitted with presumed mild to moderate DKA who were treated with the SC insulin DKA protocol between July and October 2020. We extracted demographic variables, comorbidities, DKA etiologies, time to DKA resolution and protocol completion, adverse events and protocol failures.
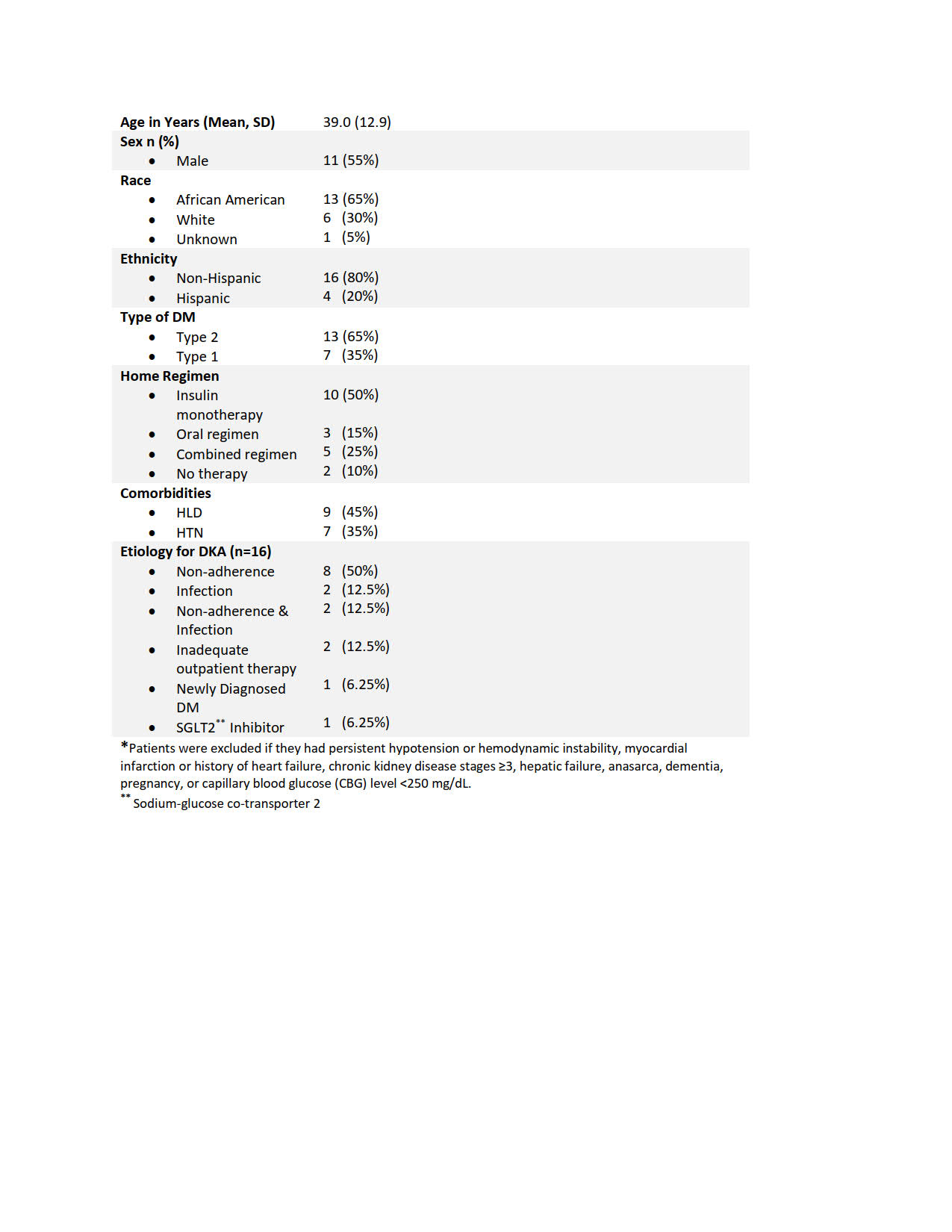
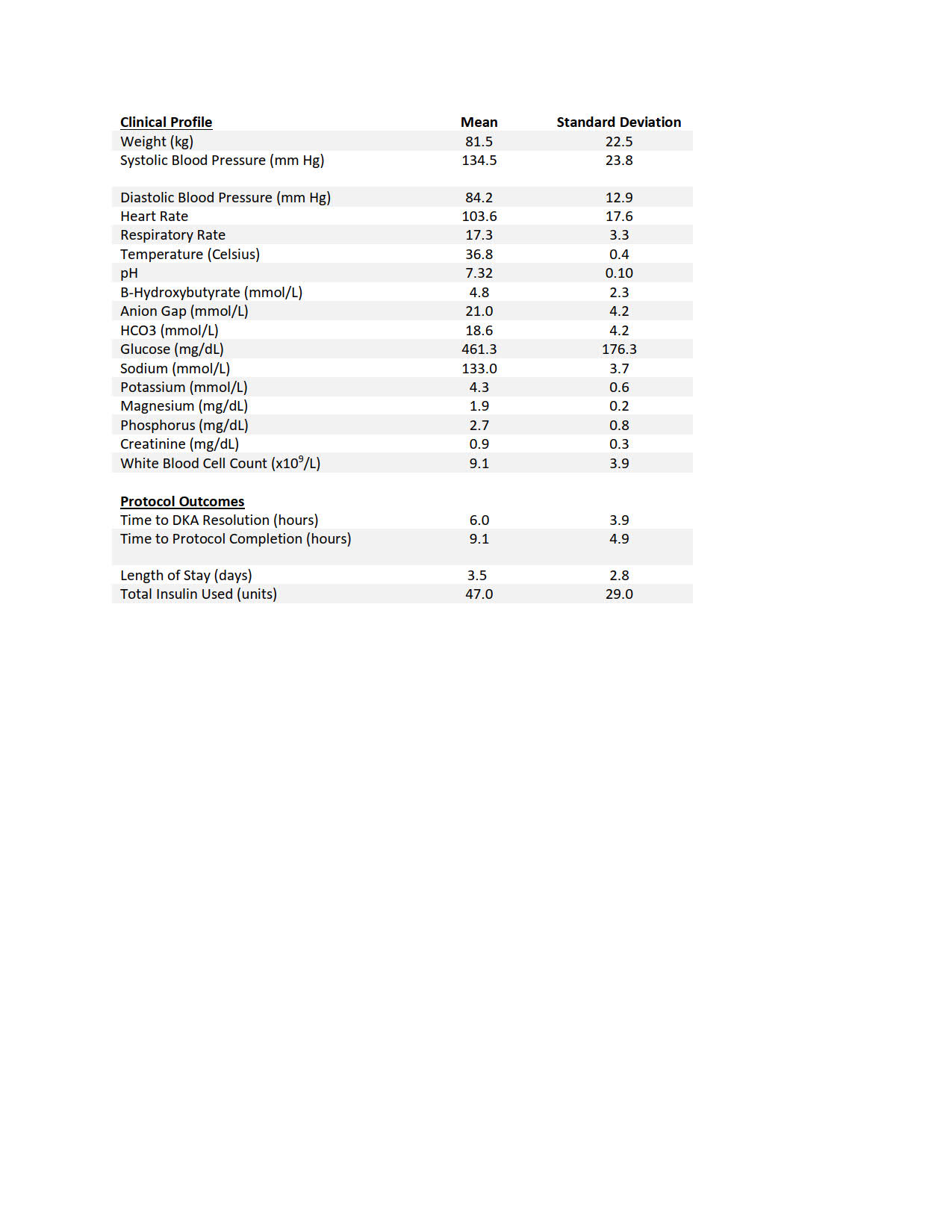
Results: A total of 20 patients were treated using the SC insulin protocol in the 4 month pilot period. Of these, 80% had mild and moderate DKA, while 20% did not meet criteria for DKA. Thirteen patients (65%) had a diagnosis of Type 2 diabetes and 7 (35%) of Type 1. The most common etiology for DKA was non-adherence with treatment (50%, 8/16), (Table 1). Mean (SD) initial CBG, anion gap, and pH were 461.3 (176.3) mg/dL, 21 (4.2) and 7.32 (0.10), respectively. Mean (SD) time to DKA resolution and protocol completion were 6.0 (3.9) hours and 9.1 (4.9) hours, respectively (Table 2). One patient was escalated to an insulin drip and three patients experienced hypoglycemia.
Conclusions: In a pilot group of patients treated with a SC DKA protocol, the use of a SC insulin regimen on a general medicine ward appears to lead to prompt resolution of the metabolic disturbance and be an adequate substitution to IV insulin therapy. No unexpected serious adverse events were reported. Critical care beds were preserved for other patients, such as those experiencing COVID-19 complications. We plan to deliver additional provider and nursing education prior to a broader rollout, in addition to redesigning the SC DKA order set to include hard stops to make sure only patients meeting the specified criteria will be treated with the SC regimen.