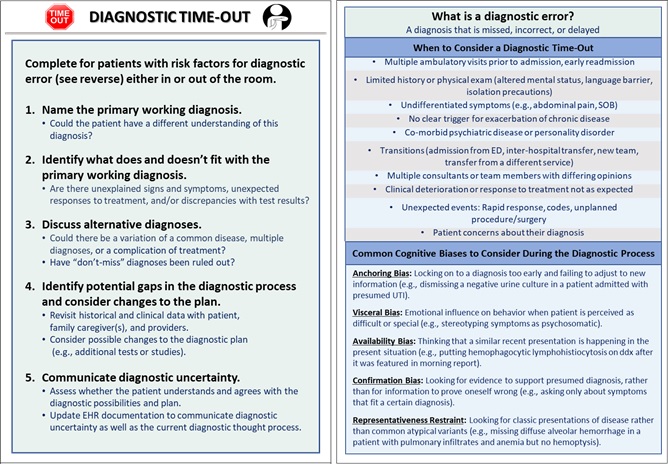
Background: The diagnostic process is fraught with diagnostic uncertainty. Typically, discussions about diagnostic uncertainty occur upon admission and during rounds, which are increasingly conducted virtually during the COVID-19 pandemic. Furthermore, key dimensions in the diagnostic process (history taking, physical examination, interpretation of diagnostic tests) are affected by breakdowns in communication between patients and clinicians, physical distancing requirements, and clinician burn-out. While educational interventions about how the diagnostic process is affected by system factors and cognitive biases are helpful, it is unclear how these strategies are perceived by learners in the current environment. As part of our AHRQ-funded Patient Safety Learning Laboratory, we developed a structured Diagnostic Time-Out (DTO; Figure 1) to encourage clinicians to acknowledge and address diagnostic uncertainty in hospitalized patients. During our implementation phase, we introduced an educational curriculum to engage clinician learners virtually in order to adhere to institutional physical distancing requirements and limited clinician bandwidth.
Purpose: We report our experience developing and conducting a virtual educational workshop aimed at introducing a DTO and creating a culture of diagnostic safety across general medicine services at a large academic medical center.
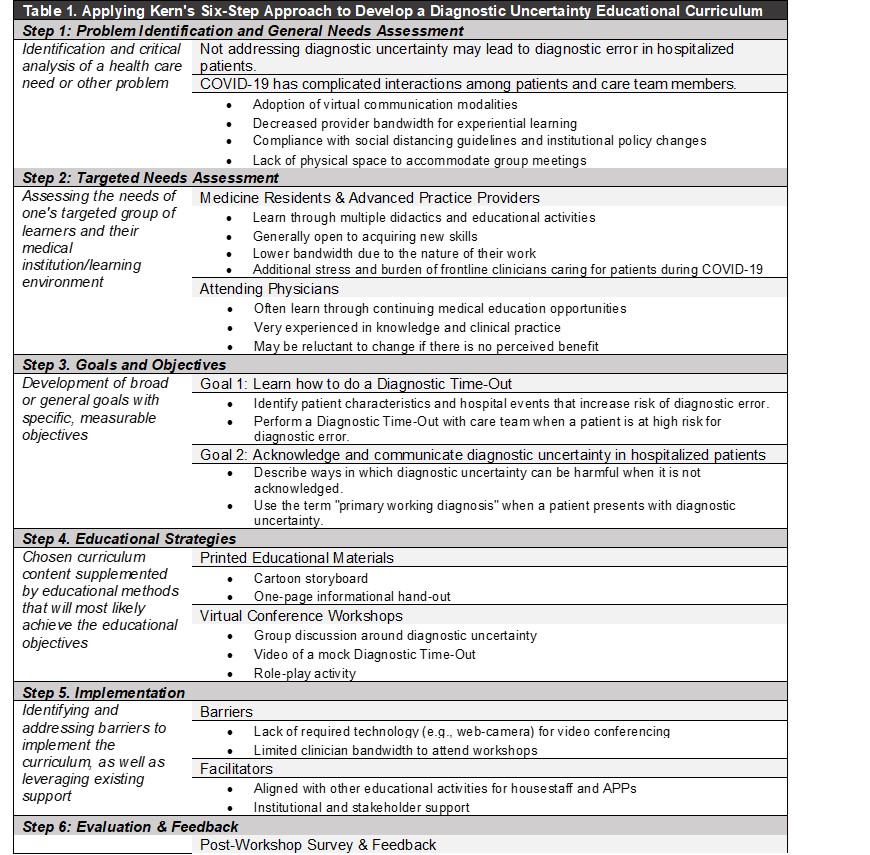
Description: To develop a curriculum, we applied Kern’s Six-Step Approach (Table 1) to address the needs of our targeted learners (advanced practice providers (APPs), house staff, attending physicians) on general medicine services. Our goals were to demonstrate to participants why and how to conduct a structured DTO and communicate diagnostic uncertainty. The components of the workshop included: 1) a brief intro using a cartoon storyboard; 2) a group discussion about diagnostic uncertainty; 3) an overview of the DTO pocket card and mobile app; 4) an overview of potential risk factors to select patients on whom to conduct the DTO; 5) a training video; and 6) an interactive role-play activity using a currently hospitalized patient selected by the team. We invited teams to our workshops via email. Materials were distributed beforehand in-person, via hyperlinks in email, and during the presentation using QR codes. To date, we have conducted eight 30-minute virtual workshops with 50 participants (12 housestaff teams, attending physicians) and solicited feedback via a web-based survey. Of the 20 survey respondents, all agreed or strongly agreed that the workshop was engaging and maintained attention; 16 (80%) stated they were likely or very likely to use the DTO in their practice. Participants commented about the lack of physical space, extreme census, lack of sufficient video/audio equipment, and constrained time as barriers to attending the workshop and/or conducting a DTO. While APPs were interested, they cited the burden of caring for COVID-19 patients during a second surge as the primary reason for not participating.
Conclusions: A multimodal approach was effective in implementing an educational curriculum to engage learners about diagnostic uncertainty for physician learners during the COVID-19 pandemic. Key barriers include insufficient technical equipment in workrooms for teams to join virtual conference sessions. Our next steps are to encourage DTO training for APPs and other healthcare professionals (e.g., nurses) when it is appropriate and their bandwidth permits.