Background: In the treatment of sepsis, current guidelines from the Surviving Sepsis Campaign recommend IV crystalloid 30ml/kg in the first three hours of admission (1). The 30mL/kg guideline is designated as a strong recommendation with low quality of evidence(2). This evidence largely stems from the Rivers et al. study of 263 patients which showed improved outcomes with early goal directed therapy (EGDT) (3). Subsequently, three larger, multicenter trials – ProMISE (n=1243), ARISE (n=1588), and ProCESS (n=1341) – failed to demonstrate a benefit with EGDT (4-6). A meta-analysis of these three trials – PRISM – failed to demonstrate a benefit (7).Consequently, the 30mL/kg fluid target has become controversial with Surviving Sepsis Guidelines citing low quality of evidence (2) and the lack of replication for EGDT benefit.The purpose of our study was to evaluate the association of achieving Surviving Sepsis Guidelines fluid targets with renal and critical care outcomes.
Methods: We conducted a retrospective single-center study of septic patients who achieved the sepsis fluid target (30mL/kg) versus patients who did not meet this target. Data were obtained from secondary analysis of an existing database that compiled patients with an ICD-10 diagnosis of severe sepsis or septic shock presenting to our tertiary care facility emergency department between January 12, 2019 and December 31, 2019. Subject inclusion: administration of vancomycin and piperacillin-tazobactam or vancomycin and cefepime within 12 hours of presentation and modified sequential organ failure assessment (SOFA) score of two or greater to meet sepsis-3 diagnostic criteria. The modified criteria use SpO2/FiO2, a validated substitute for the original SOFA standard(8). Subject exclusion: age less than 18 years, pregnancy, presenting after cardiac arrest, or current receiving renal replacement. Fluid volume was assessed in the first six hours from presentation to the emergency department. Acute kidney injury (AKI) was defined according to Kidney Disease Improving Global Outcomes (KDIGO) criteria, with omission of urine output due to poor documentation. Renal recovery was defined as a 33% reduction in serum creatinine, consistent with a proposed definition (9).
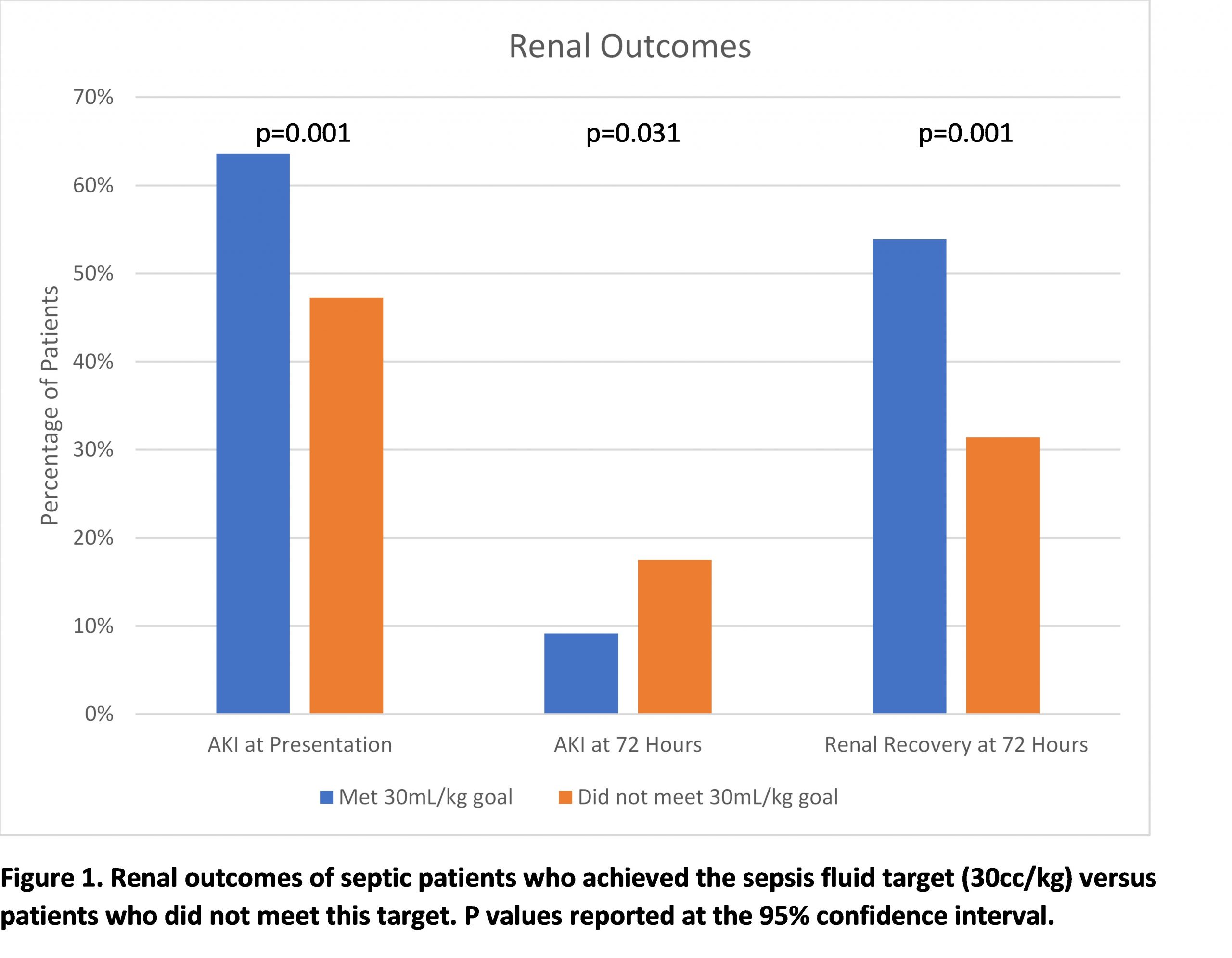
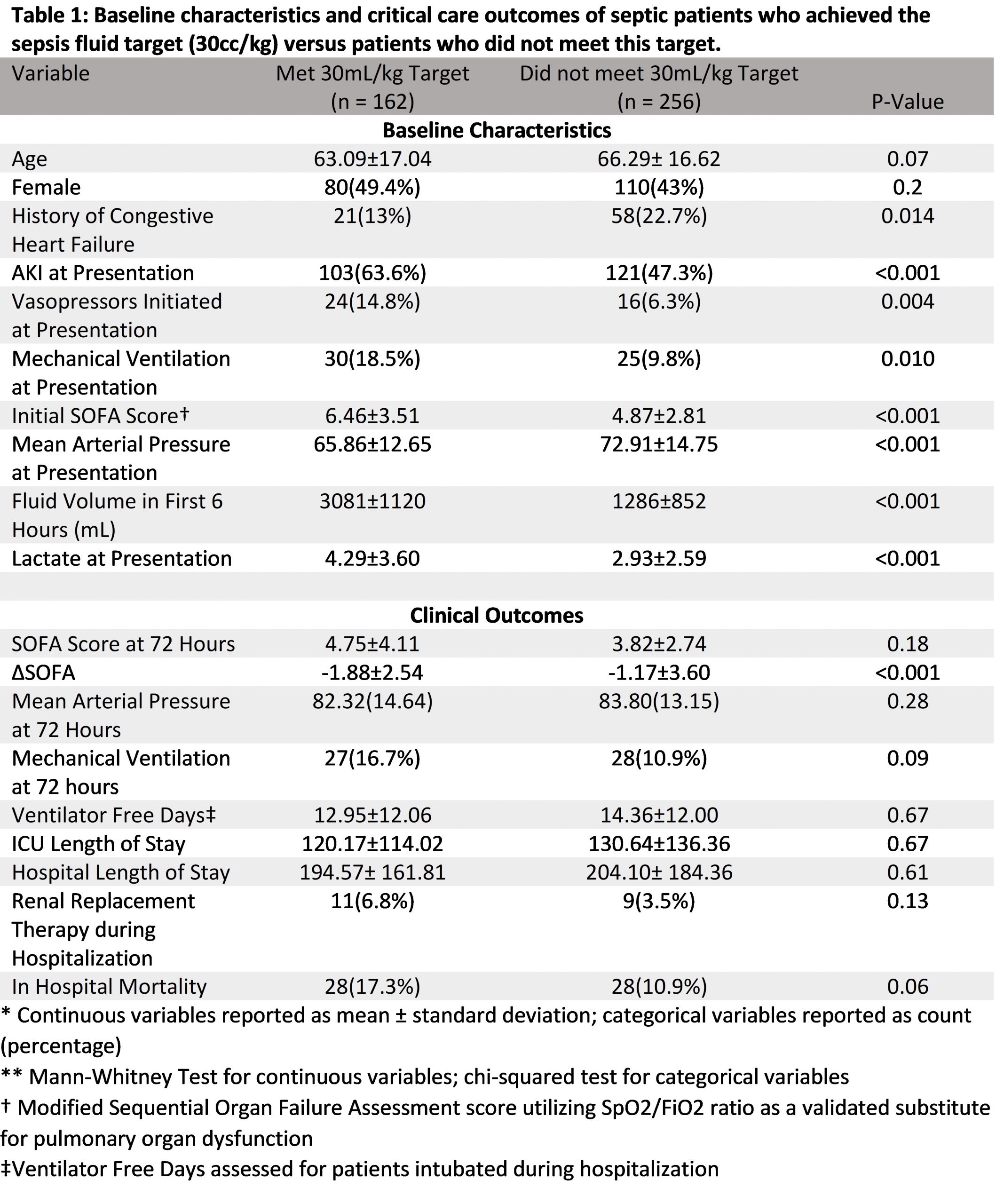
Results: A total of 418 patients were included: 162 (38.8%) met target (MT) and 256 (61.2%) did not meet target (NMT). Seventy-two percent of MT patients and forty-two percent of NMT patients experienced hypotension or lactate ≥4mmol/L at presentation. The two primary endpoints were change in modified 72-hour SOFA score and renal function. The MT group showed significantly greater improvement in mean modified SOFA score (MT = -1.88 vs. NMT = -1.17; p<0.001). The MT group showed greater improvement in kidney function with lower incidence of acute kidney injury at 72 hours and increased renal recovery (Figure 1).
Conclusions: Achieving the Surviving Sepsis Guidelines fluid target of 30mL/kg was associated with improved renal outcomes and greater 72-Hour SOFA score improvement for septic patients. Our study adds to the current conflicting literature assessing liberal vs. conservative fluid strategies by assessing a population specifically with sepsis-3 diagnoses with a focus on renal outcomes.