Background: Diagnostic errors are often attributed to cognitive and systems factors, including breakdowns in patient-clinician communication. The COVID-19 pandemic has limited this communication due to institutional infection control policies and physical distancing mandates, potentially increasing risk of diagnostic error. Virtually administered questionnaires that engage patients in assessing their experience with the diagnostic process have potential to improve diagnostic concordance among patients and clinicians and patients’ experience of care, while adhering to infection control guidelines. As part of our AHRQ-funded Patient Safety Learning Laboratory, we previously designed and piloted a 10-item questionnaire that assesses patients’ understanding of their diagnosis and satisfaction with patient-clinician communication. During our implementation phase, we modified our in-person workflow to enable virtual completion of the questionnaire by hospitalized patients.
Purpose: We report our experience administering a mobile diagnostic questionnaire to patients through a hybrid remote and in-person workflow during the COVID-19 pandemic.
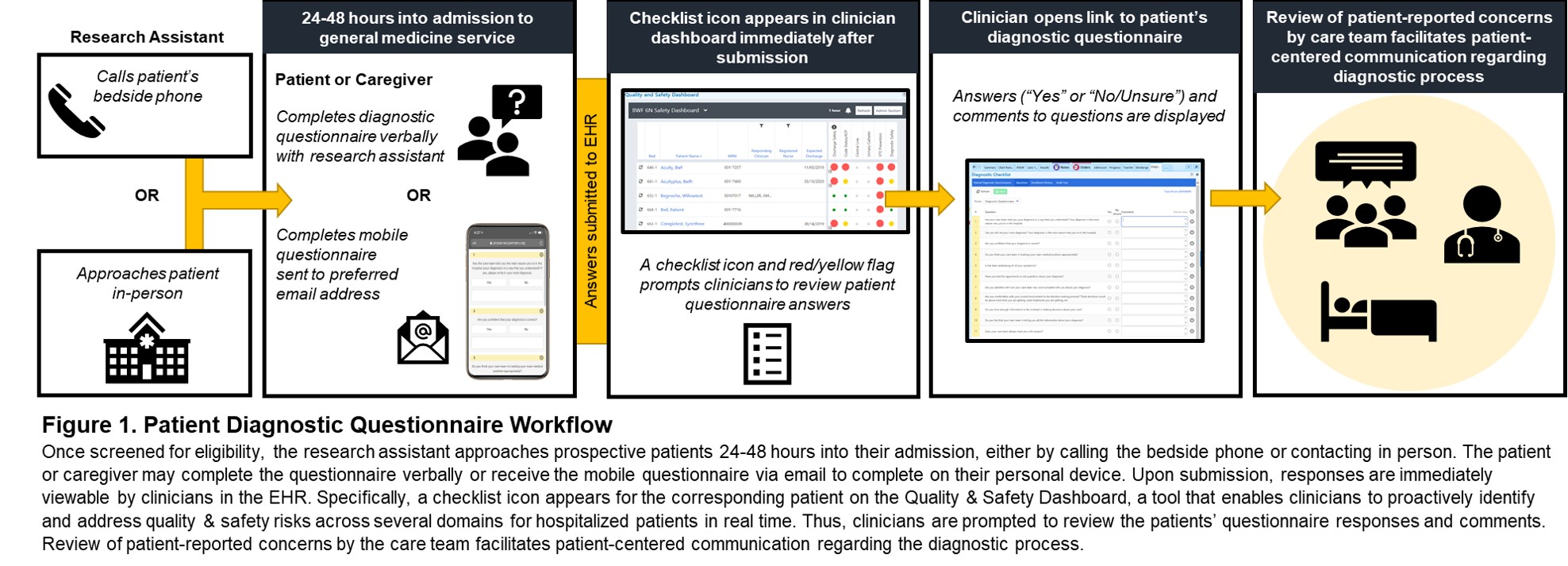
Description: All patients admitted to general medicine services were screened for eligibility (less than 48 hours into admission) via the electronic health record (EHR). Patients on enhanced precautions as well as those not on precautions, were remotely called on their beside phones. Those who were not on precautions were approached in person if they could not be reached by phone. Patients were given the option to complete the questionnaire with the research assistant, or have the questionnaire sent to their mobile device via email (prepopulated from the EHR and confirmed). All answers were available for clinicians to review in real-time via the EHR. Of 61 patients screened to date, 38 (62%) were approached via phone call or in person; the remainder were unavailable (did not pick-up call, off-unit, sleeping), in pain, approaching discharge, or surpassed the eligibility period. Of these 38 patients, 24 (63%) agreed to complete the questionnaire: 13 (54%) requested that the questionnaire be administered verbally and 11 (46%) opted for the mobile version. Of these 11 patients, 1 (9%) preferred a different email instead of the email prepopulated from the EHR, and 8 (73%) successfully completed the questionnaire on their own. The mean (SD) age of patients who opted to complete the questionnaire verbally compared to those who opted to complete the mobile questionnaire was 57 (16.54) vs. 39 (13.44) years, respectively (p = 0.012).
Conclusions: We demonstrated the feasibility of remotely administering a mobile questionnaire to engage patients in reporting their experience with diagnosis, amidst implementation constraints due to the COVID-19 pandemic. Preference for mobile questionnaire administration favored younger patients, suggesting a digital divide among older participants. Our next steps are to assess patients’ experience completing the mobile questionnaire to improve its graphical user interface and explore ways of targeting older patients or their caregivers. We plan to leverage our Quality & Safety Dashboard (Figure 1) to encourage clinicians to review their patients’ questionnaire responses, to improve diagnostic concordance and patient-clinician communication, thereby reducing risks that may contribute to diagnostic error in hospitalized patients during and after the pandemic.