Background: In tertiary care centers, transfers from outside hospitals are a common occurrence. Prior studies have shown that interhospital transfers (IHT) in certain populations are associated with an increased adjusted odds of ICU transfer (Mueller 2019). In the age of the electronic medical record(EMR), patient transfer has been improved by direct access to patient records. Prior studies have shown that shared EMRs decrease the amount of repeat testing preformed after transfer (Rome 2019). Unfortunately, hospital transfers that come from institutions with different EMRs still rely on physical copies of patient records to accompany the patient at time of transfer. Currently, at our institution, there is no standard regarding which documents are included in these packets. Instead they are compiled by various staff at the sending institution. Packets can vary from a few pages to a thick packet of records containing few clinically relevant details. In an anonymous study of internal medicine residents (n=68) that our team conducted, 79% of residents surveyed felt that critical information was usually or always missing from the provided records and 98% have needed to call for more information within 4 hours of transfer. Dissatisfaction in accompanying records has been duplicated in surveys of other tertiary care centers as well (Mueller 2019).
Purpose: Our project aims to standardize transfer documentation for IHT accepted to internal medicine services at our institution. On review of literature, the safety surrounding patient transfer is improved by improving completeness of documentation included with the patient at the time of transfer (Usher 2016). By establishing a standardized process for hospitals that frequently transfer patients to our center but do not share our EMR, we aim to improve physician satisfaction and reduce medical errors surrounding IHT.
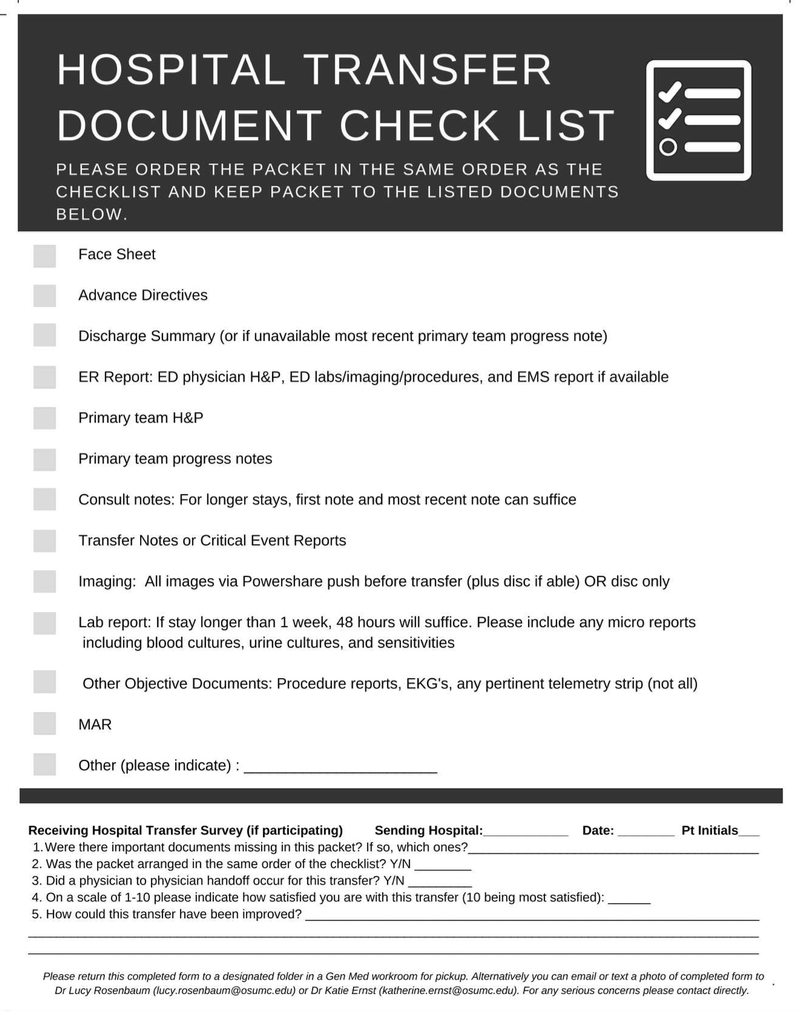
Description: We preformed focus groups with internal medicine residents, transfer center management staff, and patient transfer committees from outside hospitals that frequently transfer patients to our institution and do not share our EMR. We also met with internal medicine residents. Using input and feedback from these groups, we established a common format for transfer documentation in the form of a transfer documentation checklist. The checklist provides a format for both the order and content of a transfer packet, easing the transfer process when electronic records are not available. Both outside hospitals and residents expressed need for improvement in this area as well as satisfaction with the established checklist. Two (of a target of five) outside institutions have already implemented the checklist for all transferred patients to internal medicine services. Each checklist contains a survey for the accepting physician to fill out to assess satisfaction with included records. Of the received surveys, accepting physicians showed increased satisfaction with provided IHT documentation after implantation of the checklist.
Conclusions: While shared EMRs improve physician access to medical information during IHT, transfers that still relay on paper records often come with incomplete documentation. By creating a standardized checklist for IHT, we improved physician satisfaction surrounding hospital transfers. While we have completed our initial roll out of the transfer checklist, we are currently undergoing PDSA cycles with the goal of having 80% of IHT from participating hospitals come with the documentation checklist.