Background: Delirium is a common and serious condition affecting hospitalized patients,particularly the elderly. It is associated with poor outcomes such as prolonged hospital stays, increasedrisk of falls, and long-term cognitive impairment. Despite its impact, delirium often goes unrecognized,specially outside the ICU due to the absence of a standardized protocol for its identification andmanagement. At Lakeland Regional Health (LRH), there is currently no designated approach to detectdelirium in non-ICU patients. Implementing targeted delirium precautions is essential to reduce these adverse outcomes and improve overall patient care.
Purpose: To reduce both hospital length of stay and fall rates, alongside strengthening adherence to the hospital’s 3-2-1 mobilization protocol (mobilizing patients three times daily, brushing teeth twice daily, and bathing once daily). By advancing this initiative, our goal is to improve the early detection and prevention of delirium, enhance patient outcomes, and streamline the care and management of older adults during hospitalization.
Description: The setting for this pilot study is the B6 medical floor at Lakeland Regional Health, a 48-bed unit dedicated to the care of hospitalized adult patients. The study population includes all patientsaged 50 years and older admitted to this unit during the implementation period. This population wasselected due to their increased vulnerability to delirium and the potential benefit of early identificationand intervention within this high-risk group. This intervention will be implemented in three phases on theB6 pilot floor at Lakeland Regional Health. In Phase 1, the CAM Short assessment tool will be introducedto screen patients over 60 years of age for delirium daily. This will support timely diagnosis, improvedocumentation in patient charts, and enhance recognition of delirium. Phase 2 will involve nursing-ledimplementation of targeted prevention and management strategies, including sleep hygiene promotion,mobility, personal hygiene, and sensory support through the 3-2-1 protocol—mobilizing patients threetimes daily, brushing teeth twice daily, and bathing once daily. By standardizing these practices, nurseswill be empowered to consistently deliver essential interventions. In Phase 3, a delirium-focused powerplan will be introduced, allowing physicians to order specific nursing interventions aimed at preventingand treating delirium. The outcomes measured will include delirium rate, medications used for delirium,falls rate, and length of stay.
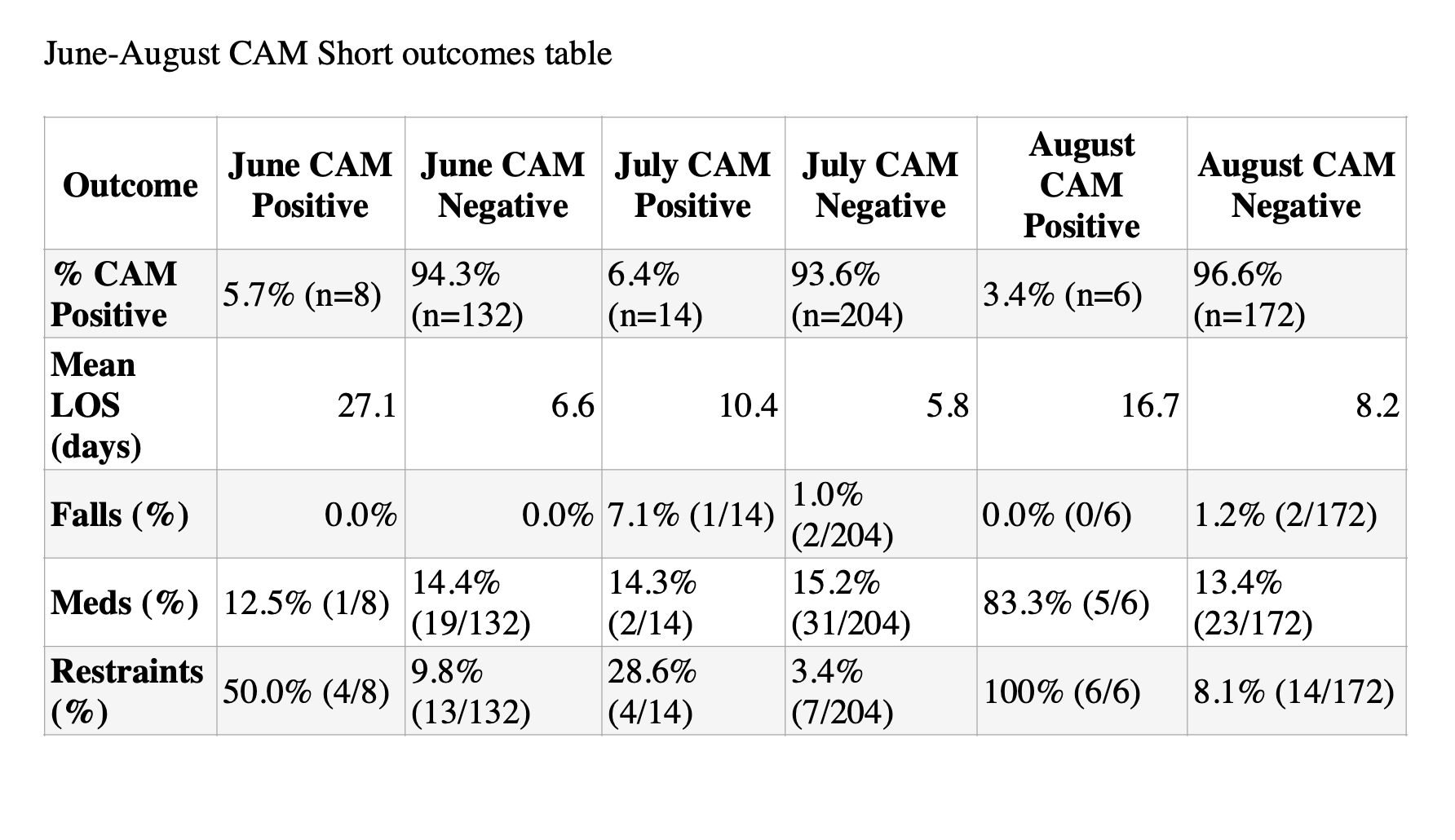
Conclusions: Over the three-month period, 536 patients over age 50 were screened with CAM Short, with 3.4%–6.4% testing positive each month. CAM Positive patients consistently had longer hospitalizations: 27.1 vs. 6.6 days in June, 10.4 vs. 5.8 days in July, and 16.7 vs. 8.2 days in August. Falls were absent in June but occurred more frequently in CAM Positive patients in July (7.1% vs. 1.0%), while August showed only falls in CAM Negative patients (0% vs. 1.2%). Medication use was similar in June (12.5% vs. 14.4%) and July (14.3% vs. 15.2%), but rose sharply in August for CAM Positive patients (83.3% vs. 13.4%), often involving antipsychotics. Restraint use remained the most striking disparity, rising from 50% in June to 28.6% in July and reaching 100% in August, compared to 3–10% in CAM Negative. These findings highlight delirium as a consistent predictor of poor outcomes and emphasize the urgent need for preventive and non-pharmacologic strategies.
.png)