Background: Substance use disorders (SUD) are a major public health concern and a major cost to the healthcare system. Patients with SUD experience higher rates of readmission, higher emergency department (ED) visits, and are less likely to receive follow up care (Peterson et al., 2021). Among veterans, only 5% of about 2.8 million diagnosed with SUD receive treatment (SAMHSA, 2024). At the Veterans Affairs Palo Alto hospital, recent data showed that 23% of patients with SUD are readmitted within 30 days, and only 53% of patients receive any follow up care after discharge.
Purpose: We aimed to improve coordination of follow-up care for medicine patients with SUD over a six-month period. Specifically, our goals were to increase (1) percentage of patients with follow-up scheduled within 30 days post discharge with general medicine clinic (GMC), addiction treatment services (ATS), or mental health clinic (MHC) by 10% and (2) the percentage of patients with SUD specialty follow-up scheduled with ATS or MHC within 30 days post discharge by 10%.
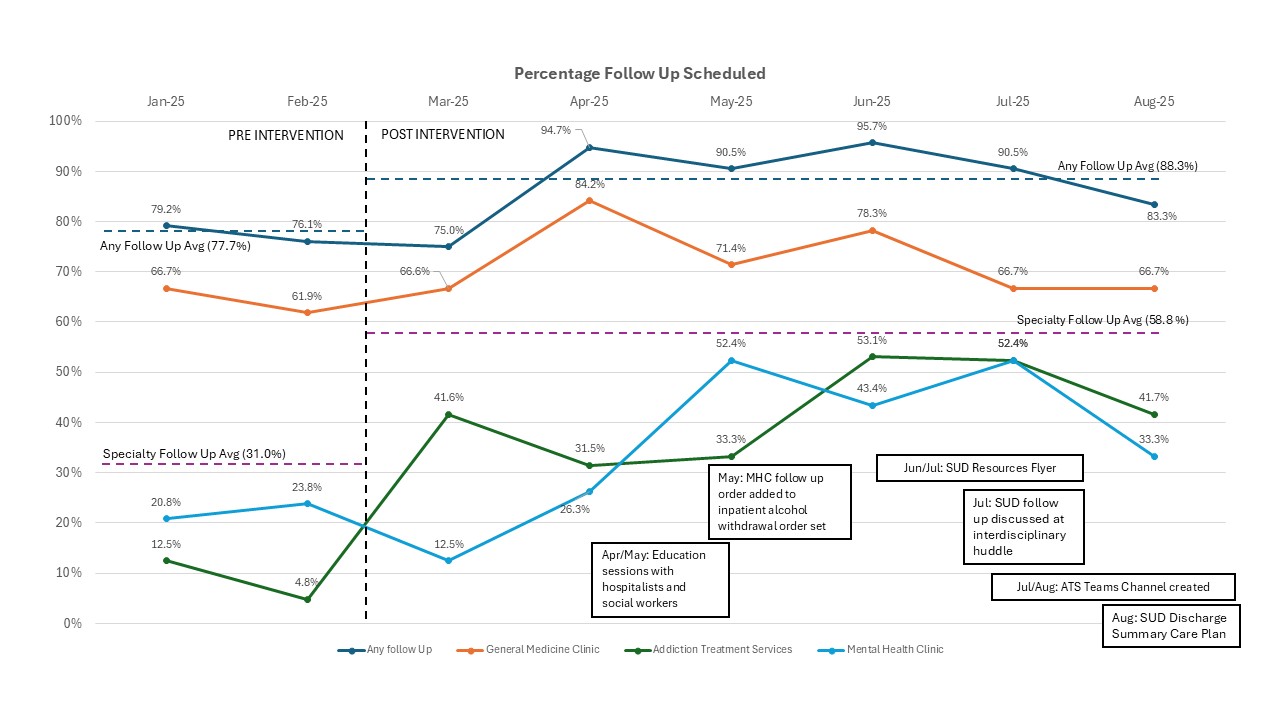
Description: Key stakeholders were engaged to develop an interdisciplinary team including inpatient medicine providers, inpatient discharge coordinators, inpatient social work, outpatient ATS, inpatient psychiatry, outpatient MHC, and inpatient SUD coordinator. Current state and gap analysis (Figure 1) revealed fragmented methods to request follow up with varying familiarity across providers, lack of direct access to schedule into ATS or MHC clinics, lack of all veterans with SUD routinely offered resources for support, limited awareness of SUD resources by providers and patients, lack of patient interest, and competing interests during hospitalization as causes of lack of SUD follow up care after discharge. In response, solutions were brainstormed and implemented by the team. To streamline follow up processes we created an ATS channel to allow real-time communication between inpatient providers and outpatient ATS team and developed a workflow for inpatient discharge coordinators to directly schedule into outpatient MHC. To improve discharge planning we leveraged daily interdisciplinary huddle to serve as a check point for SUD follow up, incorporated an SUD focused care plan as a part of the discharge summary and created an SUD focused discharge order set for medicine providers. We also developed a patient facing SUD resource flyer and conducted targeted educational sessions for social workers, residents, and hospitalists to improve awareness about available services. Rates of scheduled 30 day follow up were collected by manual review of the electronic health record. Baseline data revealed that the percentage of patients scheduled with either GMC, MHC or ATS follow up within 30 days post discharge was 77.7%. The percentage of patients with specialty SUD care within 30 days post discharge (MHC or ATS) was 31.0%. After implementation of the above interventions over a six-month period, these rates increased to 88.3% and 58.8% respectively. This represents a 13% increase in the rates of any follow up (GMC, ATS, or MHC) and 28% increase in the rates of specialty (ATS or MHC) follow up. (Figure 2)
Conclusions: Hospitals can leverage key inpatient touch points to engage patients in SUD care. Multidisciplinary collaboration and establishing strong connections with both inpatient and outpatient teams enables efficient workflows to be developed. Next steps include refining solutions and expanding successful strategies beyond the inpatient medicine service.
.jpg)