Background: Rest is essential for healing, yet hospital environments frequently disrupt sleep due to noise, clinical care interruptions, and inconsistent nighttime routines. Although evidence-based strategies to improve rest exist (1,2, 3), there is limited guidance on how to prepare clinical teams for the coordinated, system-wide implementation of Quiet at Night practices to enhance rest across inpatient units.
Purpose: Our team collaboratively planned a hospital-wide Quiet at Night initiative, using a structured implementation-science approach to translate evidence into practice. As part of the educational component, we aimed not only to implement the program but also to learn from the process. During our educational sessions, we collected survey data from team members to better understand their perceptions of the project’s acceptability, appropriateness, perceived effectiveness, and feasibility. These insights helped us evaluate the initiative in a systematic way while strengthening our team’s ability to apply evidence-based strategies in future quality-improvement efforts.
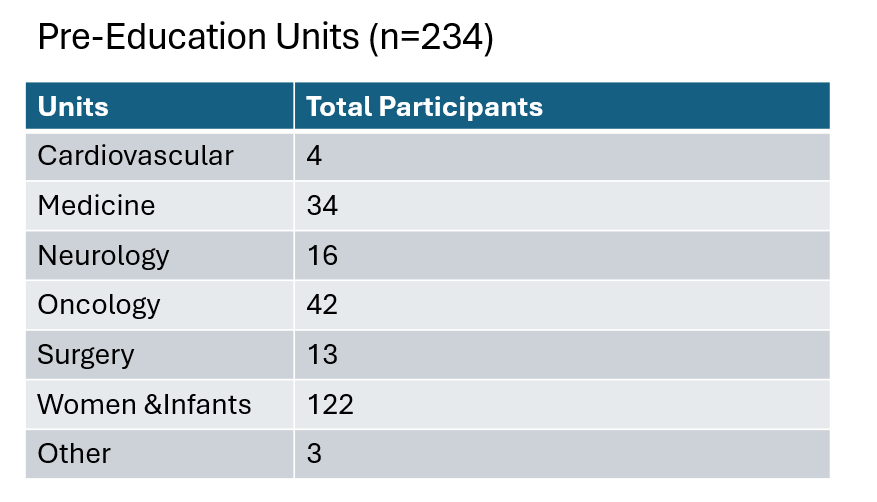
Description: Our Quiet at Night initiative was developed through close collaboration with nursing leadership, Hospital Medicine, Patient Experience, and our research team. Our group began by mapping nighttime workflows including timing of lab collection, medication administration, and vital signs, and reviewed hospital-wide patient experience data regarding nighttime rest and disruptions. We identified modifiable disruptions and designed a standardized Quiet at Night bundle that included clustered care, environmental modifications (sleep kits, ear plugs), and communication strategies to set expectations with patients and families. After IRB approval, we prepared the project for implementation. To support unit-level customization, we partnered with frontline nursing teams, patient care technicians, lab services, and environmental services to identify workflow barriers and operationalize quiet hours. We also delivered standardized education to nursing leaders and frontline care providers on each pilot unit. During education sessions, 234 participants (78% RN, 12% PCT, 10% other) completed a pre-education survey on existing night-time practices. Although most (80%) described their unit as fairly quiet, 70% rated overall patient rest as fair or poor. Following instruction on the Quiet at Night bundle, 193 participants (81% RN, 11% PCT, 8% other) completed a post-education survey. Seventy-seven percent reported the education prepared them to better support patient rest, and 70% endorsed the interventions as acceptable, appropriate, efficacious, and feasible.
Conclusions: A structured, interdisciplinary implementation strategy improved clinician readiness for change and supported the perceived feasibility of a system-wide Quiet at Night initiative. Early endorsement of the intervention’s acceptability and appropriateness suggests strong potential for sustained adoption. Limitations include use of site-specific survey instruments and potential selection bias. These findings highlight the importance of interdisciplinary planning, leader engagement, frontline involvement, and deliberate preparation when implementing rest-promoting practices across a large health system.
.png)