Background: Hospitals are facing increasing admission denials from insurance companies while simultaneously managing limited resources due to ongoing financial pressures and the residual effects of the COVID-19 pandemic. Patients are also experiencing growing frustration with rising out-of-pocket costs and unnecessary hospitalizations that can lead to additional copayments and hospital acquired conditions (HACs).
Purpose: To address these challenges, we developed an innovative proof-of-concept pilot program to:1. Ensure patients requiring hospital services receive timely, appropriate care.2. Prevent inappropriate admissions for patients who could be managed in outpatient settings.3. Improve accuracy of admission status upfront to minimize costly rework.4. Provide targeted education and feedback to Emergency Department (ED) providers on admission practices and use of outpatient resources.
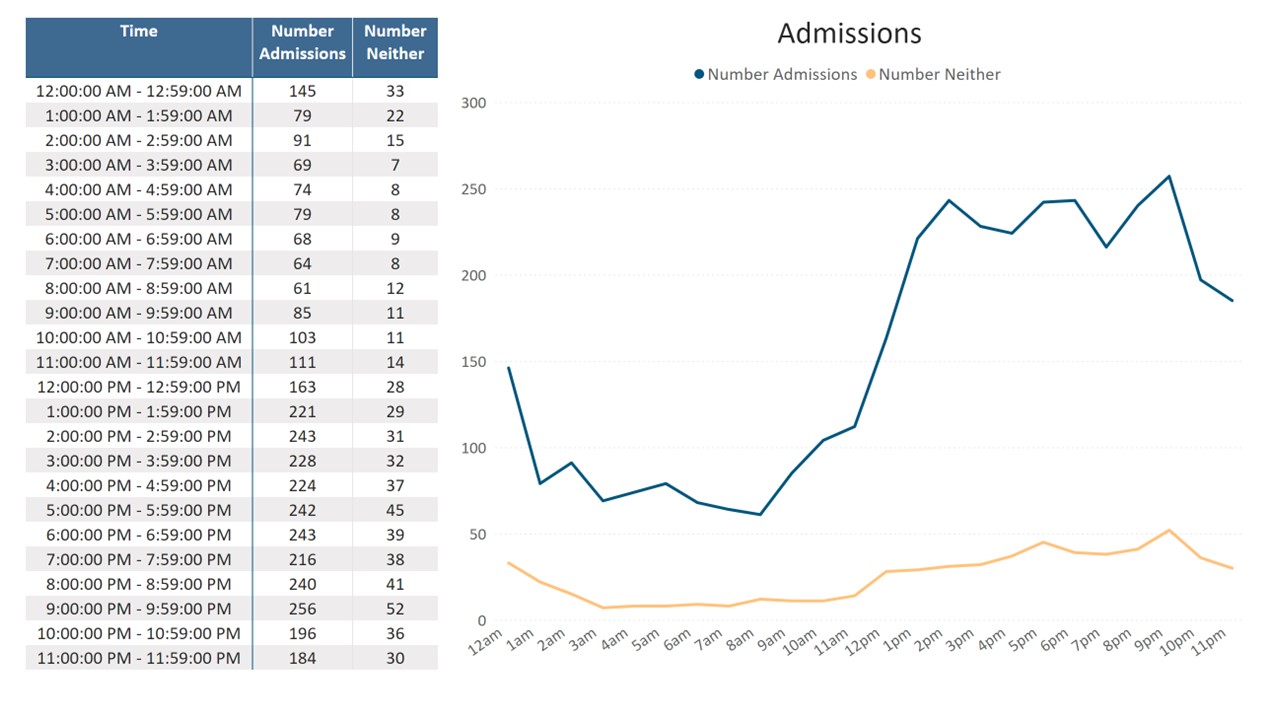
Description: The pilot leveraged InterQual, a nationally recognized screening tool commonly used by hospitals and insurers to evaluate the medical necessity of inpatient and observation care. Stakeholders included Emergency Medicine (EM) providers, admitting providers, physician advisors, and Utilization Review (UR) nurses. Admission requests were tracked by ED provider, capturing:1. Total admission requests2. Proportion meeting inpatient level of care (LOC)3. Proportion meeting observation LOC4. Requests not meeting any LOCProvider level data were compared against encounter volumes, with outliers flagged for targeted education.Initial training for ED and admitting providers focused on medical necessity criteria, correct admission status assignment, and use of outpatient alternatives when appropriate. The UR nurses conducted real-time preadmission “Initial Reviews” in InterQual, with all communication facilitated through Epic Secure Chat. Results were reported after 6 weeks to the ED Medical Director. Provider specific statistics and peer comparisons were shared. One-on-one education was delivered to ED providers with higher-than-expected admission rates and lower acuity case patterns. Admission patterns were evaluated including trends around shift changes, throughput delays, and ED discharge opportunities.
Conclusions: This process with enhanced accountability improved ED discharge processes, documentation quality, and timeliness of care. This avoided denials and improved throughput. The hospital identified opportunities for process change to facilitate ED discharges, improve documentation, improve timeliness of care in the ED, avoid boluses of admissions, and create accountability. There was a 16% improvement in patients meeting inpatient LOC following targeted education and feedback. 88% of patients who met inpatient LOC via Initial Review were ultimately discharged as inpatients without concurrent authorization denials. Overall, the number of admissions (inpatient and outpatient observation) decreased by 3-4 patients daily over historical averages. Kaiser Family Foundation estimates that hospitals spend $3000 per patient day (1). By ensuring only patients who need hospital care are admitted, this process is estimated to save $3-4 million annually ($3000 * 3-4 patients * 365 days).
.jpg)