Background: Hospital medicine – orthopedic surgery co-management programs can improve postoperative outcomes and efficiency. Rising surgical volume at Stanford Health Care Tri-Valley, a community academic hospital affiliated with Stanford University, created a need for a structured approach to managing complex joint arthroplasty patients. To meet this demand and optimize resource use, the hospital medicine and orthopedic teams developed an advanced practice provider (APP) – led co-management model. The program began in 2023.
Purpose: We designed a formal co-management process for patients undergoing total hip or knee arthroplasty who require inpatient monitoring due to case complexity or comorbidities. The program aimed to (1) increase capacity for orthopedic surgical growth, (2) improve postoperative monitoring for increasingly complex patients, and (3) leverage hospitalist APP expertise while balancing admitting demands for attending hospitalists.
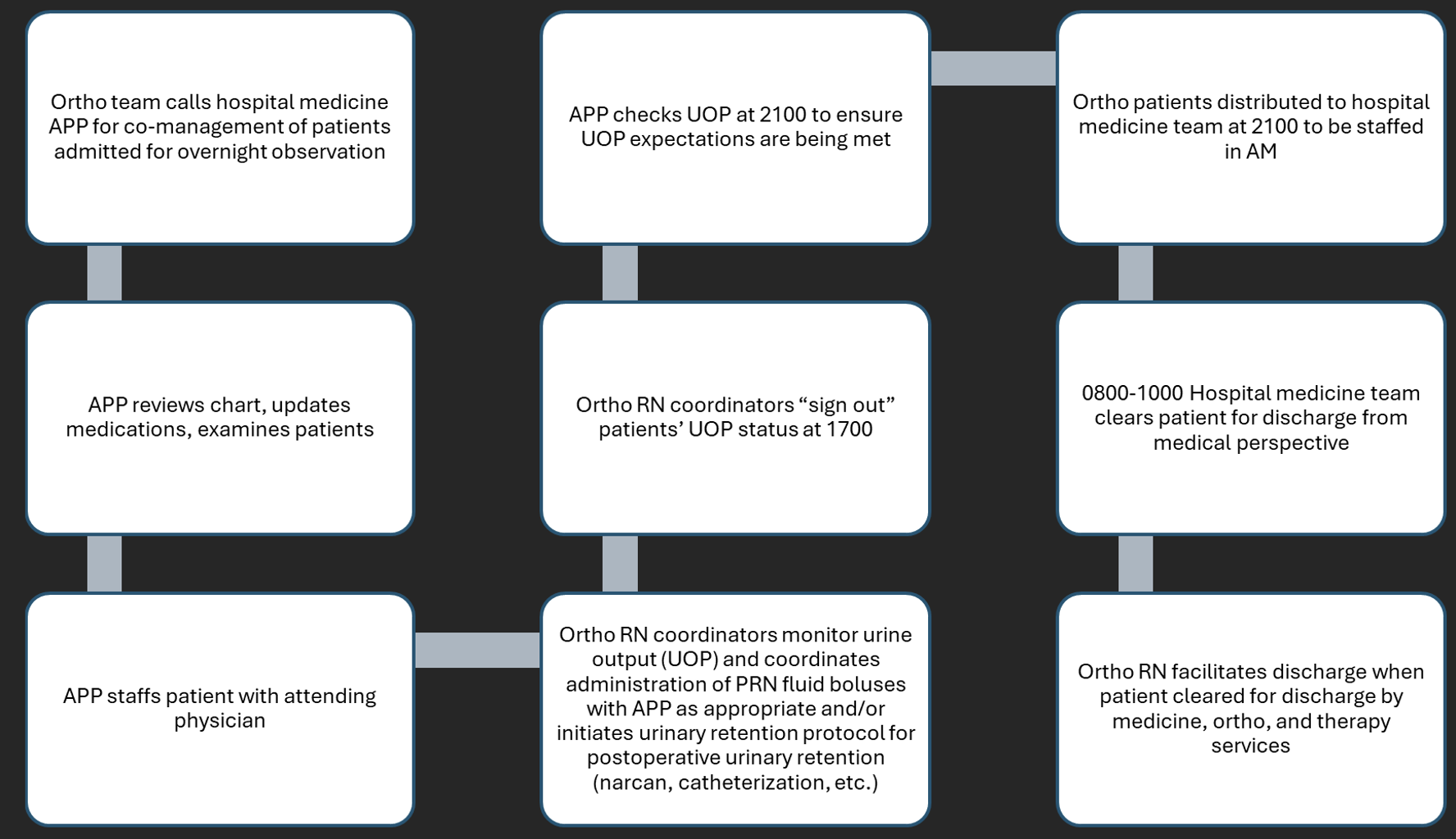
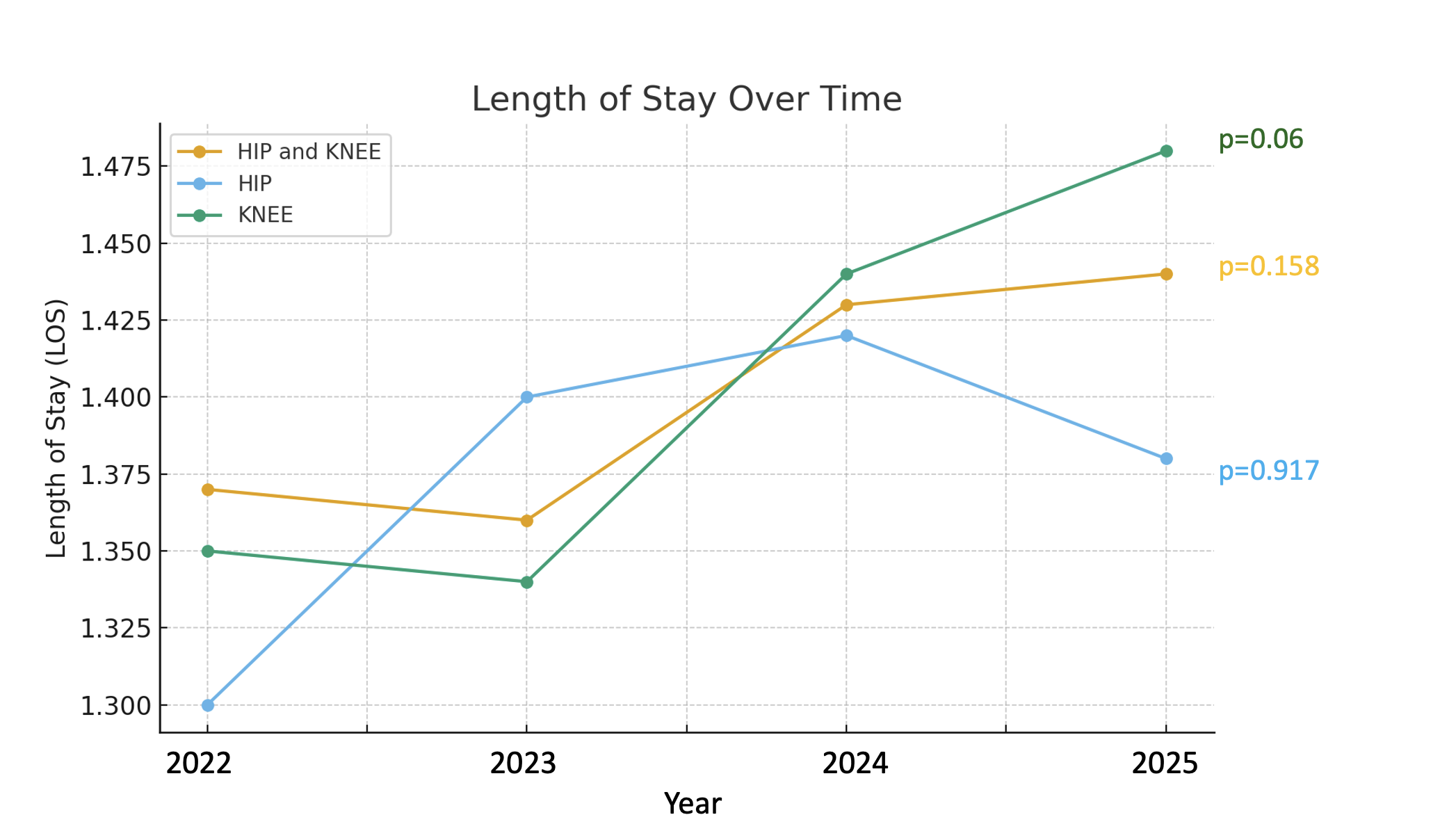
Description: The co-management program consisted of four phases:• Care transition: Orthopedic surgeons, APPs, or nurse coordinators provide a sign-out to the hospital medicine team upon transfer to the PACU.• Medical management: Hospitalist APPs, with an attending hospitalist, optimize postoperative medications and manage medical complications.• Nursing and therapy coordination: Orthopedic nurse managers and APPs monitor urine output as a proxy for volume status and track postoperative milestones. PT/OT evaluations and early ambulation begin on POD0.• Discharge process: Both orthopedic and medical teams evaluate patient prior to 9am and use secure messaging to facilitate discharge before noon.Outcomes data were obtained from Epic and included all patients admitted after total joint procedure from September 2022 to September 2025. Outcomes were analyzed on an annual basis, and included length of stay (LOS), complication rate, and MS-DRG weight (indicating medical complexity of patients). Total joint arthroplasty cases increased by 60.9%, from 248 in 2022 to 399 in 2025 (total hip arthroplasties increased by 55% from 100 to 155; total knee arthroplasties increased by 64.9% from 148 to 244). 90.6% of cases were outpatient or observation level of care. We tracked complications included DVT/PE, AKI, hyponatremia, acute hypoxia, heart failure exacerbation, and surgical site infection. The overall complication rate was 1.6% across 2022–2025, with a peak of 3.2% in 2025. Hyponatremia accounted for 61.5% of complications, increasing from 1 case in 2022 to 10 cases in 2025, which was not statistically significant (p=0.069). Rates of other complications remained negligible. Length of stay (LOS) from 2022 to 2025 did not significantly change (average LOS 1.41 days, p=0.158).
Conclusions: The APP-led orthopedic co-management model has enabled substantial surgical growth and improved discharge efficiency. Most importantly, we have maintained low complication rates while accommodating more complex patients, as suggested by increased MS-DRG weight, without adversely affecting LOS or complication rates. The statistically insignificant increase in hyponatremia corresponded with AI-assisted documentation improvements, suggesting that coding accuracy may explain part of the trend. Overall, this co-management program demonstrates that APP-driven co-management can safely expand surgical throughput, optimize inpatient care, and strengthen collaboration between hospital medicine and surgical services in community academic settings.