Background: Diagnostic errors are common in U.S. hospitals. About six in ten adults who have experienced a medical error encountered a missed, delayed, or incorrect diagnosis. Miscommunication between the patient and care team likely contributes to these errors. Engaging patients in assessing their understanding of the diagnosis may improve diagnostic accuracy as well as the patients’ experience of care. As part of our AHRQ-funded Patient Safety Learning Laboratory, we are analyzing the problem of diagnostic error in acute care with the goal of designing and developing solutions that engage patients in the diagnostic process.
Purpose: We report the process of designing, developing, and pilot testing a patient-centered diagnostic questionnaire that assesses patients’ understanding of their diagnosis and their satisfaction with communication about the diagnostic process with their care team.
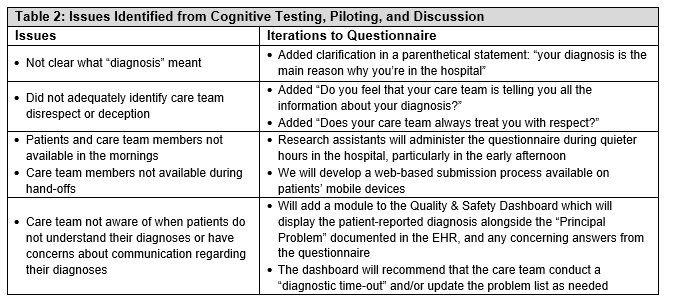
Description: We drafted questions to assess the failures in communication around the diagnostic process identified by our systems and human factors engineers. The eleven-item questionnaire (Table 1) assesses patients’ understanding of their admission diagnosis and confidence that it is correct; whether all their symptoms are being addressed; their experience and satisfaction with care team communication about their diagnosis; and their involvement in shared decision-making. We performed cognitive testing on nine patients, asking them if they understood the questions and if they could restate the questions in their own words. We then conducted a short pilot during which we administered the questionnaire to patients admitted to general medicine units. Of 78 patients approached, 39 patients (50%) agreed to complete the questionnaire; the remainder were unavailable (e.g. off-unit, sleeping), in pain, upset, or near discharge. Of 39 participants, 22 (56.4%) answered yes to all questions (i.e., had no concerns); 29 (74.4%) were confident about their diagnoses; and 32 (82.1%) affirmed that they had enough information to be involved in shared decision-making. The patient-reported diagnosis was concordant with the patient’s “Principal Problem” entered in the electronic health record (EHR) in 18 of 39 (46.2%) cases. Based on input from patients and stakeholders, we refined the questions and identified potential strategies for incorporating the questionnaire into clinical workflow (Table 2).
Conclusions: We pilot tested, iteratively refined, and demonstrated the feasibility of administering a questionnaire that engages patients in reporting their concerns about the diagnostic process during hospitalization. We observed gaps in patients’ understanding of their main diagnoses and poor concordance between patients’ understanding of their diagnoses and the clinical team’s EHR documentation. Main challenges include offering patients more convenient ways to complete the questionnaire, incorporating responses into clinical workflow to ensure that the care team addresses them, and re-administering the questionnaire on patients who reported concerns. We plan to address these challenges by developing a mobile, web-based application for patients to submit the questionnaire; we also plan to leverage our EHR-integrated Quality and Safety Dashboard to report questionnaire results in real-time and recommend that care team members conduct a structured “diagnostic time-out” and/or update the “Principal Problem” on the EHR problem list.